Introduction
(Article introduction authored by Conquest Editorial Team)
The kidney is crucial for filtering waste from the body, with renal transplantation being the primary treatment for end-stage renal failure.
Graft dysfunction, like acute rejection, poses a challenge to transplant survival. Renal biopsy is the gold standard for diagnosis but is invasive and costly.
Noninvasive imaging techniques are being researched as alternatives. Chronic kidney disease (CKD) affects millions, with transplants improving outcomes.
However, post-transplant complications, especially graft dysfunction, remain concerning. Current diagnostic methods like glomerular filtration rate (GFR) and renal biopsy have limitations. This paper aims to discuss current clinical techniques for renal transplant evaluation and explore new image-based methods for detecting graft dysfunction.
Treatment
Luckily, there have been developments in treatments for patients with stage 5 renal failure. Those treatments include blood dialysis or renal transplant. Blood dialysis is when one’s blood is filtered of waste or excess water, either with use of a machine outside the body (hemodialysis) or chemically inside the body (peritoneal dialysis).
Though dialysis is a helpful treatment, a longer-term treatment would be kidney transplantation. This is where a donor’s kidney is surgically inserted into the CKD patient.
That new kidney should improve filtration for the patient. Since transplantation is the definitive therapy for End-Stage Renal Disease (ESRD), the following describes in more
Transplantation
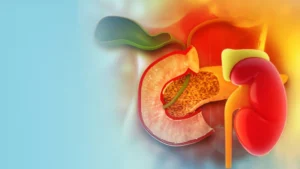
Renal transplantation involves placing a donated kidney into a patient with CKD, typically without removing the patient’s malfunctioned kidneys unless necessary.
The donated kidney is positioned below the native kidneys, with its ureter connecting to the bladder and its artery and vein connecting to the patient’s iliac vessels. Fig. 1 demonstrates the entire anatomy of a patient’s renal system after transplantation.
Finding a suitable donor can be complex, with options including living and cadaver donors. Living donors must meet specific criteria, and cadaver donors must have functioning kidneys at the time of death.
Despite around 17,000 kidney transplants performed annually in the US, there are approximately 100,800 people awaiting a kidney. Therefore, it’s crucial to maintain the viability of the transplanted kidney to avoid further surgeries. Post-transplantation care focuses on follow-up procedures and managing complications for transplant patients.

Post-transplant follow-ups and complications
After renal transplantation, patients must undergo regular follow-up appointments to monitor kidney function and prevent complications like infection and bleeding.
They should adhere to their physician’s instructions, including taking anti-rejection medications and attending scheduled visits. Initially, visits are frequent but decrease over time.Clinical assessments during appointments involve monitoring weight, blood pressure, and temperature. If abnormalities arise, further tests like renal biopsy or scans may be ordered to assess kidney health.
This article focuses on complications associated with renal transplants, particularly graft dysfunction, while also discussing other potential issues.
Types of complications
There are 6 categories of complications including: urological complications, vascular complications, fluid collection, recurrent native renal disease, graft dysfunction, & neoplasms.
Graft dysfunction
Graft dysfunction occurs when the newly transplanted organ ceases to function, leading to toxin buildup and rejection by the body. Around 15% of patients experience graft dysfunction within the first 5 years post-transplantation.
There are three classes of graft dysfunction: hyperacute, acute, and chronic. Hyperacute rejection, though rare, is caused by antibodies attacking the organ due to HLA or ABO incompatibility.
Chronic rejection typically occurs after 5 years post-transplant. This article focuses on acute kidney rejection (AKR), which has various causes including acute tubular necrosis, antibody-mediated rejection, T-cell mediated rejection, immunosuppressive toxicity, and viral infection.
Each cause requires specific treatment, which can pose challenges in diagnosis and management.
The causes of AKR may occur singularly or in combination, complicating diagnosis. Diagnostic methods for identifying these causes will be discussed in the following section of the article.
Chronic rejection typically occurs after 5 years post-transplant. This article focuses on acute kidney rejection (AKR), which has various causes including acute tubular necrosis, antibody-mediated rejection, T-cell mediated rejection, immunosuppressive toxicity, and viral infection.
Each cause requires specific treatment, which can pose challenges in diagnosis and management. The causes of AKR may occur singularly or in combination, complicating diagnosis. Diagnostic methods for identifying these causes will be discussed in the following section of the article.
Detection/assessment of renal rejection
Regular visits with a physician are crucial to ensure the proper functioning of a newly transplanted organ. The main goal of post-transplantation follow-up is to maintain the viability of the graft for as long as possible.
By attending regular follow-ups and promptly reporting any symptoms, patients can potentially detect problems early and preserve the donated organ. This article provides an overview of techniques for diagnosing graft dysfunction, including traditional non-imaging clinical methods and image-based techniques, which are still under development or improvement. Further details on both methods are provided below.
Traditional methods
Traditionally, during a routine follow-up a blood and urine analysis will be implemented. If there are any abnormal results in either of these, the physician may order a renal biopsy to get a definitive diagnosis.
This diagnosis should also tell the physician what is causing the kidney malfunction. This next section will show how these diagnoses are determined. First, this article will discuss urine testing.
Urine tests
Urine tests are simple and non-invasive, allowing physicians to measure biomarkers to determine Glomerular Filtration Rate (GFR). Serum creatinine is often used as a biomarker, and GFR is calculated using an equation with constants adjusted for sex, race, and age. This helps determine kidney function stage, with 0 indicating increased risk and 5 indicating end-stage renal failure. While suggested by the National Kidney Foundation, urine tests have limitations such as low sensitivity and late-stage marker detection. They also do not assess individual kidney function. The next diagnostic test to be discussed is a blood test.

Blood test/works
Blood tests for estimated GFR, similar to urine analysis, use serum creatinine but are slightly more invasive as they require a blood sample. A complete blood count (CBC) and differential count (diff) detect substances beyond urine, including burr cells indicative of CKD.
Burr cells, resembling gear-like structures, indicate elevated waste levels in the body, common in CKD patients.
While blood analysis offers additional benefits, it shares limitations with urine tests, including low sensitivity and late-stage marker detection, and does not assess individual kidney function. The next traditional method to be discussed is renal biopsy.
Biopsy (“Gold Standard”)
Renal biopsy is a traditional method for the graft function assessment that is by far the most invasive, but to date is considered the gold standard.
This procedure is performed using a renal biopsy needle that is inserted into the patient’s back and kidney while being guided by a camera, ultrasound, or X-ray, as shown in Fig. 2.
The tissue that is obtained is read using a microscope. The patient is fully conscious and told not to move; if one should move, they run the risk of piercing other organs.
Along with the risk of piercing other organs the patient also runs the risk of excessive bleeding and infections. Excessive bleeding can present itself more so in a patient who is on blood thinners.
Infections are likely to occur since the patient is more than likely on an immunosuppressive therapy regimen. These complications can lead to nephrectomy or even death; both occur in 1 in every 1000 renal biopsies.
Image-based techniques for renal transplant evaluation
Non-invasive imaging-based techniques are gaining attention for renal transplant assessment, with computer-aided diagnosis (CAD) systems being actively researched.
Imaging modalities like radionuclide imaging offer qualitative and quantitative assessment of graft function and complications but lack precise anatomical information and involve radiation exposure.
Computed tomography (CT) provides accurate evaluation but lacks specificity for detecting acute renal rejection and involves nephrotoxic contrast agents. Ultrasound (US) and magnetic resonance imaging (MRI) are popular for diagnosing kidney diseases, with MRI being more costly but offering superior imaging.
This survey will explore CAD systems for diagnosing acute renal rejection using US and MRI.superior imaging. This survey will explore CAD systems for diagnosing acute renal rejection using US and MRI.
Ultrasound (US) imaging
Ultrasound (US) imaging is usually used for the early assessment of renal allografts functionality in the postoperative period as well as for the assessment in the long-term follow-up due to being a relatively easy to be performed and repeated, inexpensive, and non-nephrotoxic imaging modality.
Pulsatility index (PI) and resistance index (RI) are the most common measurements to assess renal functionality using US.
Below, we will discuss some recent studies that assessed renal transplants using different forms of ultrasound (e.g., power Doppler (PD), color Doppler (CD), contrast enhanced (CE), etc.) as shown in Fig. 3.
Although several studies utilized US to evaluate and assess renal functionality pre- and post-transplantation by evaluating conventional ultrasound parameters, for instance the PI and RI, two contradictory studies concluded that RI is not an exact sign of renal graft dysfunction, and it could only offer a predictive marker of the graft.
Moreover, Doppler US may give high RI and PI values (>0.8), which is an indication comparable to those of ATN. These contradictions led researchers and investigators to examine a different imaging modality to assess renal functionality (e.g., MRI). In the next section, we will discuss up-to-date studies utilizing different MR imaging modalities.

Magnetic resonance imaging (MRI)
Magnetic resonance imaging (MRI) is a non-ionizing technique widely utilized for its superior soft tissue contrast and morphological information. Unlike other imaging methods like ultrasound (US) and computed tomography (CT), MRI offers detailed analysis of renal function. MRI includes specific scans that provide both structural and functional information, such as dynamic MRI, BOLD MRI, and diffusion MRI. Recent studies have employed these MRI modalities for assessing renal transplant functionality.
Dynamic contrast-enhanced (DCE) MRI
Renal dynamic MRI (DCE-MRI) is an emerging technique for evaluating kidney function. It involves repeated imaging before and after contrast agent administration.
Several studies have utilized DCE-MRI to assess both native and transplanted kidneys, characterizing functional parameters like renal blood flow (RBF), glomerular filtration rate (GFR), and renal plasma flow (RPF).
For instance, de Priester et al. used dynamic MR enhancement curves to distinguish between diseased and nondiseased renal transplants. Other studies developed CAD systems based on DCE-MRI for transplant function evaluation, achieving high diagnostic accuracy.
However, concerns over nephrogenic systemic fibrosis with contrast agents in DCE-MRI have led to exploration of alternative MRI modalities like DW-MRI and BOLD-MRI for renal transplant assessment.
Blood oxygen level dependent (BOLD) MRI
In addition to DCE-MRI, another imaging technique, called BOLD-MRI, has been utilized to study renal rejection using the amount of oxygen diffused blood (i.e. oxygen bioavailability) in the kidney determine if it is functioning properly. Specifically, the amount of deoxyhemoglobin is measured by the apparent relaxation rate (R2) parameter (Fig. 4)

BOLD-MRI has been explored for assessing renal allografts. Studies by Djamali et al. and Han et al. examined BOLD-MRI’s ability to differentiate between normal allografts and those with dysfunction (AR and ATN).
Both found decreased MR2 values in dysfunctional allografts, but Han et al. also observed higher MR2 values in AR compared to normal allografts.
Sadowski et al. similarly found decreased MR2 values in AR allografts. Liu et al. investigated BOLD-MRI’s utility in detecting renal allograft rejection, observing the lowest MR2 values in AR cases. However, BOLD-MRI faces challenges due to low SNR, electromagnetic field weaknesses, and limitations related to kidney motion and susceptibility induced by bowel gas, impacting image quality.
Diffusion-weighted (DW) MRI
DW-MRI has garnered attention for renal function assessment due to its ability to offer both anatomical and functional information without radiation exposure or contrast agent administration.
Studies by Eisenberger et al., Hueper et al., and Xu et al. utilized DW-MRI to assess renal allograft function, observing decreased ADC values in dysfunctional allografts, particularly in cases of acute rejection.
Vermathen et al. explored long-term stability and changes in renal allografts using DW-MRI, while Katarzyna et al. investigated relationships between diffusion parameters and laboratory results post-transplantation.
Several studies, including those by Abou-El-Ghar et al. and Liu et al., aimed to distinguish between normal renal allografts and those with dysfunction, such as acute cellular rejection (ACR) or acute tubular necrosis (ATN), achieving significant differentiation based on ADC values.
Shehata et al. conducted studies to classify renal transplant status and identify rejection types using DW-MRI, achieving high classification accuracies. DW-MRI shows promise for non-invasive assessment of renal allograft function, but challenges remain, including variations in ADC values and susceptibility to motion artifacts.
MRI with specific contrast agent (ultrasmall superparamagnetic particles of iron oxide “USPIO”)
Ultrasmall Superparamagnetic Particles of Iron Oxide (USPIO) is a contrast agent utilized in MRI, potentially useful for diagnosing renal rejection by detecting macrophage presence in the kidney. USPIO’s signal weakens as more macrophages absorb the particles, indicating kidney stress and rejection. Although promising in rat models for preclinical renal rejection diagnosis, USPIO lacks specificity and cannot determine the reason for macrophage presence. Larger animal studies may be the next step to validate USPIO’s safety and efficacy before considering human trials.
Conclusion
Though the treatment of chronic kidney disease has improved greatly with the use of transplants, there are still challenges such as graft dysfunction that provide a challenge in maintaining survival of the new organ. In the future, the use of image-based diagnosis will be improved and implemented in the diagnosis of both pre- and post-transplantation.
It is hoped that by having these improved imaged based CAD systems that diagnosis of graft dysfunction will be less invasive, more accurate, time saving, and inexpensive compared to renal biopsies and other traditional methods of diagnosis. By having all of these advantages it is expected that graft survival will improve in cases of graft dysfunction.
References
1. A. Kukla, M. Adulla, J. Pascual, M. Samaniego, L. Nanovic, B.N. Becker, et al. CKD stage-to-stage progression in native and transplant kidney disease Nephrol Dial Transplant, 23 (2) (2008), pp. 693-700
2. About chronic kidney disease; 2016 [cited 2016 May 2, 2016]. Available from: https://www.kidney.org/kidneydisease/aboutckd
3. Foundation NK. Organ donation and transplantation statistics; 2016 [cited 2016 May 25 2016]. Available from https://www.kidney.org/news/newsroom/factsheets/Organ-Donation-and-Transplantation-Stats
4. G.L. Myers, M.G. Miller, J. Coresh, J. Fleming, N. Greenberg, et al. Recommendations for improving serum creatinine measurement: a report from the laboratory working group of the national kidney disease education program
5. Dialysis; March 1, 2012 [cited 2016 May 3, 2016]. Available from: http://www.niddk.nih.gov/health-information/health-communication-programs/nkdep/learn/living/kidney-failure/dialysis/Pages/dialysis.aspx
6. M. Desai, I.S. Gill Laparoscopic surgery in renal transplant recipients C.M. Mobley, S.J. Pelletier
7. Current procedures: surgery R.M. Minter, G.M. Doherty (Eds.), Current procedures: surgery, McGraw-Hill, New York (NY) (2010)Urol Clin N Am, 28 (4) (2001), pp. 759-767
8. A.C. Gruessner Schwartz’s principles of surgeryC. Brunicardi (Ed.), Schwartz’s principles of surgery, Mcgraw-Hill, New York (NY) (2014) 9. A.C. Gruessner Schwartz’s principles of surgery C. Brunicardi (Ed.), Schwartz’s principles of surgery, Mcgraw-Hill, New York (NY) (2014)
10. The national waiting list; 2016. [Web Page] December 2015 [cited 2016 April 14, 2016]. Available from: http://www.transplantliving.org/before-the-transplant/getting-on-the-list/the-national-waiting-list/.
11. NK Foundation NKF: care after kidney transplant Available from: http://www.kidney.org/atoz/content/immunosuppression (2015)
12. Hospital SCs. Kidney: clinic and follow-up visits after kidney transplantation; 2016 [cited 2016 May 18, 2016]. Available from http://www.seattlechildrens.org/clinics-programs/transplant/kidney/clinic-followup-visits-after-kidney-transplantation/.