
Introduction
Due to the optimal results obtained in kidney transplantation and to the lack of interest of the industries, new innovative drugs in kidney transplantation are difficult to be encountered. The best strategy to find the new drugs recently developed or under development is to search in the sections of kidney transplantation still not completely covered by the drugs on the market. These unmet needs are the prevention of delayed graft function (DGF), the protection of the graft over the long time and the desensitization of preformed anti human leukocyte antigen antibodies and the treatment of the acute antibody-mediated rejection. These needs are particularly relevant due to the expansion of some kind of kidney transplantation as transplantation from non-heart beating donor and in the case of antibody-incompatible grafts. Second, some of these drugs are still in an early phase of study, even if in well-conducted randomized controlled trials. Indeed, is always necessary to verify whether the study is still going on or whether and why the study itself was abandoned. Drugs for unmet therapeutic needs. These drugs may be categorized as follows:
(1) Therapy for ischemia-reperfusion injury (IRI) that results in delayed graft function (DGF);
(2) Therapy to preserve optimal kidney function over the long-term; and
(3) Therapy for desensitization and antibody-mediated rejection (ABMR).
Therapy for DGF
Acute kidney injury (DGF) occurs in the first week of transplantation. DGF is associated with increased immune activation, complement activation and release of damage-associated molecular patterns. Several drugs to treat DGF have been tried, many of them failed to prove their effectiveness. However, new drugs have recently emerged and they are still in randomized controlled trials (RCTs) to control DGF.
Anti-apoptotic strategies
Apoptosis plays an important role in shaping DGF. QPI-1002 also known as 15 NP, is a short interfering RNA that inhibits the expression of p53. Pro-apoptotic gene p53 is activated by hypoxia and induces cell cycle arrest and apoptosis. However, RCT was terminated in 2018 without positive results because of a lack of documented efficacy.
Pegylated carboxyhemoglobin
Carbon monoxide (CO) is involved in regulating endothelial cell survival and proliferation. It also plays roles in protecting against DGF through IRI, vessel relaxation and inhibition of proinflammatory responses. CO is a very powerful anti-apoptotic substance and has anti-inflammatory effects. The use of pegylated carboxyhemoglobin is currently the object of a phase 2/3 study to analyze the efficacy and safety of SANGUINATE for reducing the DGF rate in patients receiving a kidney transplant.
Relaxin
In DGF, relaxin (RLX) has an anti-inflammatory effect by reducing the expression of intracellular adhesion molecule 1. RLX causes vasodilatation through increased NO production and inhibition of endothelin 1 production. Two studies documented improved renal function, histologic improvement in damaged tissue after DGF.
Hepatocyte growth factor
Angel-3777, formerly BB3, is a hepatocyte growth factor mimetic that binds to its transmembrane tyrosine kinase receptor, cMET. In preclinical studies, it exerts anti-inflammatory and regenerative effects. It may also be effective when administered after AKI-related DGF.
Complement inhibition
Complement activation plays a significant role in IRI, which causes and precedes DGF. Mirocept inhibits C3/C5 convertases and C1 esterase inhibitors. This drug may also be administered as a donor pretreatment strategy in high-risk recipients.
![]()
Improving perfusion techniques
Improving perfusion techniques is not drugs in the sense of the word but rather a different strategy to prevent IRI and DGF. It was documented that active oxygenation during hypothermic machine perfusion is the most beneficial in cases involving the use of DCD kidneys when applied starting from kidney procurement until transplantation. Active oxygenation improves preservation and subsequent early graft function.
Therapy to preserve renal function
These drugs may be divided into the following categories:
(1) Therapy to avoid nephrotoxicity, usually by elimination of calcineurin inhibitors (CNIs);
(2) Therapy to control inflammation and fibrosis (principally when inflammation overlaps fibrosis); and
(3) Therapy to prevent donor-specific antibodies (DSAs) and treat chronic ABMR (cABMR).
Therapy to avoid nephrotoxicity
induced by CNIs
The complete withdrawal of CNIs is difficult to achieve and is only appropriate for low-risk patients and donors. The use of belatacept or other agents blocking the costimulatory pathways is the other method to avoid CNIs. Everolimus efficacy was demonstrated, but low-dose tacrolimus was needed.
Therapy to control inflammation and
fibrosis not related to immunological
causes
Several factors, such as hyperuricemia, glucose intolerance, arterial hypertension, dyslipidemia and infection, may induce an inflammatory state in kidney transplant patients. IL-6 leads to allograft injury by acute inflammation, adaptive cellular/humoral responses, innate immunity and fibrosis. Several drugs have been proposed to control the graft inflammatory state, including low-dose aspirin, statins, renin-angiotensin inhibitors, and xanthine-oxidase inhibitors. The most often studied is tocilizumab, anIL-6R blocker, which increased Tregs and reduced T effector cytokines in renal graft inflammation.
Therapy to control chronic humoral
rejection
Clazakizumab is a humanized monoclonal antibody directed against IL-6. It has shown promising results in patients with cABMR, which is a slowly progressing disease in which grafts are primarily injured by de novo DSAs. A study by Dobere et al. reduced DSAs and demonstrated beneficial effects on cABMR and renal function.
Therapy for desensitization and acute
ABMR
Desensitization is the treatment to reduce or, when possible, completely eradicate DSAs before or at the time of transplant. Treatment of ABMR includes powerful drugs aimed at controlling this severe complication. Naïve CD4+ T cells recognize the antigen presented by APCs. Costimulatory molecules mediate the presentation through CD80/86 and CD28. Obintuzumab is a type 2 anti-CD20 antibody that induces more robust B cell depletion than RTX. Belimumab belongs to the anti BAFF family and is effective in treating systemic lupus erythematosus. Isatuximab is effective on PCs and other immune cells, such as Tregs and Bregs.
To better understand the mechanism of action of these drugs, Figure 1 represents how DSAs are formed and where the immunosuppressant drugs may act

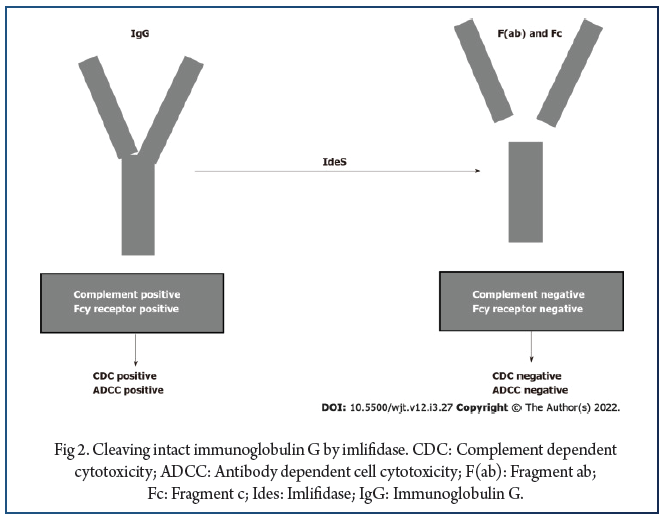
In ABMR, the activation of the complement cascade is triggered by ligation of the C1 complex to HLA antigens. Several drugs are capable of blocking complement activation. Antibody removal is another therapeutic technique that may be applied primarily to desensitize patients with preformed DSAs. Humanized monoclonal antibody eculizumab binds to C5 with high affinity and prevents C5 convertase-mediated cleavage to C5a and C5b. In the past, several studies documented the efficacy of eculizumab in treating ABMR. Recently, other studies documented the efficacy of eculizumab in treating and preventing ABMR. Antibody removal is another therapeutic technique that may be applied primarily to desensitize patients with preformed DSAs before transplantation. Until recently, antibody removal and/or inhibition have been performed by plasmapheresis and IVIGs. Recently, it was documented that imlifidase (IdeS), a recombinant cysteine protease derived from Streptococcus pyogenes, rapidly cleaves IgG in the lower hinge region to a Fab fragment and a dimeric Fc fragment (Figure 2).
Conclusion
Examining unmet needs in the field of kidney transplantation may help us to find new drugs. Needs not optimally covered by current drugs are control of DGF, long-term immunosuppression with graft outcomes reduced by chronic damage and the control of desensitization and ABMR. In the first kind, controlling or reducing DGF is essential; in the latter kind, the reduction of antibodies against HLA is essential. DGF may be controlled either with optimal management of the donor before or during kidney removal or with drugs attempting to target one of the multiple pathways involved in causing the IRI that is conducive to DGF.New drugs are also emerging to control or reduce the antibody serum level. Several steps are involved in antibody generation and for each of those steps new drugs will be found. In addition, drugs are able to reduce the nephrotoxicity induced by the long-term use of CNIs and to control kidney inflammation that may contribute to a worse graft outcome. Therefore, trials with novel agents require a careful approach and these new agents in transplantation face many challenges, but may provide a hopeful pipeline in this issue.
References:
1. Viklicky O, Novotny M, Hruba P. Future developments in kidney transplantation. Curr Opin Organ Transplant. 2020;25:92–98.
2. Siedlecki A, Irish W, Brennan DC. Delayed graft function in the kidney transplant. Am J Transplant. 2011;11:2279–2296.
3. Rosin DL, Okusa MD. Dangers within: DAMP responses to damage and cell death in kidney disease. J Am Soc Nephrol. 2011;22:416–425.
4. Moll UM, Zaika A. Nuclear and mitochondrial apoptotic pathways of p53. FEBS Lett. 2001;493:65–69.
5. Orlando G, Remuzzi G, Williams DF. Kidney Transplantation, Bioengineering and Regeneration. In: Chandran S, Vincenti F. Novel Drugs in Kidney Transplantation in Kidney Transplantation. New York: Elsevier, 2017: 277-290.
6. Tchervenkov J, Squiers E, Stratta R, Odenheimer D, Rothenstein D QPI-1002 DGF Study Group. QPI-1002, a siRNA Targeting p53: Improvement in Outcomes Following Acute Kidney Injury (AKI): Cardiac Surgery to AKI Donors. Am J Transplant. 2017;17.
7. Schutt R, Case J, Barrick B, Toll A, Schaffer R, Fisher J, Marsh C. Living kidney transplant: the influence of intra-operative hemodynamics on delayed graft function. 2017 American Transplant Congress; 2017 Apr 29-May 3; Chicago, USA.
8. Ruan Y, Wang L, Zhao Y, Yao Y, Chen S, Li J, Guo H, Ming C, Gong F, Chen G. Carbon monoxide potently prevents ischemia-induced high-mobility group box 1 translocation and release and protects against lethal renal ischemia-reperfusion injury. Kidney Int. 2014;86:525–537.
9. Kohmoto J, Nakao A, Stolz DB, Kaizu T, Tsung A, Ikeda A, Shimizu H, Takahashi T, Tomiyama K, Sugimoto R, Choi AM, Billiar TR, Murase N, McCurry KR. Carbon monoxide protects rat lung transplants from ischemia-reperfusion injury via a mechanism involving p38 MAPK pathway. Am J Transplant. 2007;7:2279–2290.
10. Hanto DW, Maki T, Yoon MH, Csizmadia E, Chin BY, Gallo D, Konduru B, Kuramitsu K, Smith NR, Berssenbrugge A, Attanasio C, Thomas M, Wegiel B, Otterbein LE. Intraoperative administration of inhaled carbon monoxide reduces delayed graft function in kidney allografts in Swine. Am J Transplant. 2010;10:2421–2430.
11. Abuchowski A. SANGUINATE (PEGylated Carboxyhemoglobin Bovine): Mechanism of Action and Clinical Update. Artif Organs. 2017;41:346–350.
12. Pharmaceuticals P. Efficacy and Safety of SANGUINATE™ for Reduction of Delayed Graft Function in Patients Receiving a Kidney Transplant. [accessed 2015 Jul 3]. In: ClinicalTrials.gov [Internet]. Bethesda (MD): U.S. National Library of Medicine. Available from: https://clinicaltrials.gov/ct2/show/NCT02490202. Clinical- Trials.gov Identifier: NCT02490202.
13. Thuillier R, Delpy E, Matillon X, Kaminski J, Kasil A, Soussi D, Danion J, Sauvageon Y, Rod X, Donatini G, Barrou B, Badet L, Zal F, Hauet T. Preventing acute kidney injury during transplantation: the application of novel oxygen carriers. Expert Opin Investig Drugs. 2019;28:643–657.
14. Steichen C, Giraud S, Bon D, Barrou B, Badet L, Salamé E, Kerforne T, Allain G, Roumy J, Jayle C, Hannaert P, Hauet T, Thuillier R. Barriers and Advances in Kidney Preservation. Biomed Res Int. 2018;2018:9206257.
15. Kaminski J, Hannaert P, Kasil A, Thuillier R, Leize E, Delpy E, Steichen C, Goujon JM, Zal F, Hauet T. Efficacy of the natural oxygen transporter HEMO2 life® in cold preservation in a preclinical porcine model of donation after cardiac death. Transpl Int. 2019;32:985–996.
16. Jakubauskiene L, Jakubauskas M, Leber B, Strupas K, Stiegler P, Schemmer P. Relaxin Positively Influences Ischemia-Reperfusion Injury in Solid Organ Transplantation: A Comprehensive Review. Int J Mol Sci. 2020;21.
17. Kageyama S, Nakamura K, Ke B, Busuttil RW, Kupiec-Weglinski JW. Serelaxin induces Notch1 signaling and alleviates hepatocellular damage in orthotopic liver transplantation. Am J Transplant. 2018;18:1755–1763.
18. Alexiou K, Wilbring M, Matschke K, Dschietzig T. Relaxin protects rat lungs from ischemia-reperfusion injury via inducible NO synthase: role of ERK-1/2, PI3K, and forkhead transcription factor FKHRL1. PLoS One. 2013;8:e75592.
19. Yoshida T, Kumagai H, Kohsaka T, Ikegaya N. Relaxin protects against renal ischemia-reperfusion injury. Am J Physiol Renal Physiol. 2013;305:F1169–F1176.
20. Collino M, Rogazzo M, Pini A, Benetti E, Rosa AC, Chiazza F, Fantozzi R, Bani D, Masini E. Acute treatment with relaxin protects the kidney against ischaemia/reperfusion injury. J Cell Mol Med. 2013;17:1494–1505.
21. Weidner KM, Sachs M, Birchmeier W. The Met receptor tyrosine kinase transduces motility, proliferation, and morphogenic signals of scatter factor/hepatocyte growth factor in epithelial cells. J Cell Biol. 1993;121:145–154.


