Introduction
Chronic kidney disease (CKD) affects a significant number of individuals worldwide and is projected to become a leading cause of death in the future. The shortage of kidney donors and the complications associated with dialysis have resulted in suboptimal treatment for end-stage renal disease (ESRD) patients. However, there have been recent developments in nephrology that hold promise for the field. These include advancements in kidney imaging, improved methods for estimating renal function, and emerging therapeutic approaches such as wearable artificial kidneys, xenotransplantation, stem cell-derived therapies, bioengineering models, and new medications. It is important to note that not all CKD patients will progress to the stage of requiring renal replacement therapy, as some may die from other causes before reaching that point. However, for those who do require treatment, innovative approaches and medications such as sodium-glucose cotransporter 2 (SGLT2) inhibitors and mineralocorticoid receptor antagonists (MRAs) hold particular promise.
Novel diagnostic methods
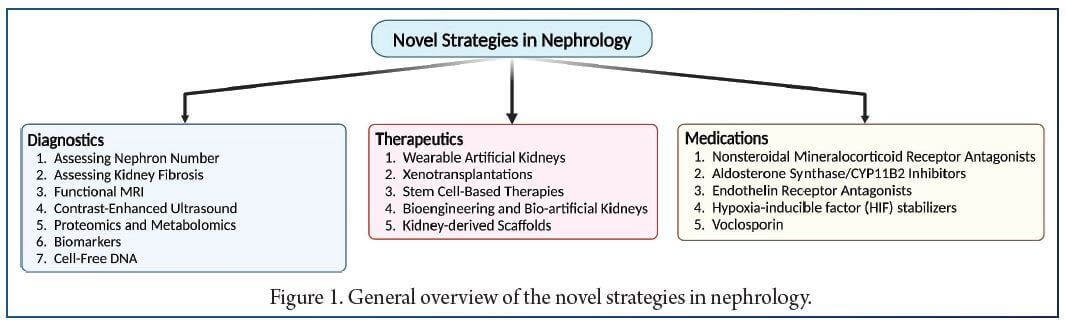
Current diagnostic methods for CKD often result in late-stage diagnosis, necessitating the development of novel approaches to enable early detection. The blind spot lies in the subclinical stage of CKD progression, where patients may exhibit no obvious signs of disease but are still at risk. Researchers are investigating imaging techniques and biomarker assessment to overcome this diagnostic challenge and provide a means for earlier detection of CKD (Fig. 1)
Imaging: assessing nephron number as a determinant of kidney disease and kidney fibrosis
Imaging techniques have emerged as valuable tools in the field of nephrology, offering non-invasive and repeatable methods for diagnosing and monitoring chronic kidney disease (CKD). These techniques provide a comprehensive assessment of kidney structure and function, allowing for early detection and evaluation of disease progression. Advancements in imaging modalities such as functional magnetic resonance imaging (MRI) and ultrasound have shown great promise. One area of focus is the estimation of nephron number, which is crucial for understanding kidney health and disease susceptibility. Novel technologies like cationized ferritin-enhanced MRI (CFE-MRI) enable non-destructive measurement of nephron number in vivo, providing valuable clinical biomarkers. Nephron number assessment can help predict CKD onset, evaluate recovery after acute kidney injury, assess donor organs, predict graft survival, and inform drug dosing and toxicity testing. Other imaging techniques, including sodium MRI, diffusion-weighted MRI, blood oxygenation level-dependent MRI, perfusion MRI, hyperpolarized carbon 13 MRI, and contrast-enhanced ultrasound, offer insights into various aspects of kidney function, fibrosis assessment, and lesion characterization. These modalities provide information on renal microstructure, tissue oxygenation, blood flow, and water handling, contributing to improved management of kidney disease. While the potential of these imaging methods is promising, further research is needed to establish their safety, efficacy, and integration into routine clinical practice. Once validated, these novel diagnostic tools have the potential to transform the field of nephrology, enabling early detection, accurate monitoring, and personalized treatment strategies for patients with CKD.
Biological fluid biomarkers
Proteomics and metabolomics have recently been tested in the field of nephrology with intriguing and promising results. Both RNA and DNA in biological fluids may serve as biomarkers. These biomarkers should correlate well with kidney disease, histopathology, progression, outcomes or early disease, and allow for rapid, noninvasive and specific measurements with high sensitivity and specificity.
Proteomic and metabolomic analysis for the detection of biomarkers
Researchers Pontillo and Mischak identified 273 urinary peptides called CKD273, using capillary electrophoresis- mass spectrometry (CE-MS), that distinguish between chronic kidney disease (CKD) patients and healthy individuals. These peptides, including collagen fragments and proteins related to inflammation and tissue repair, outperformed traditional markers in predicting and diagnosing CKD. Another study introduced the Kidney Risk Inflammatory Signature (KRIS), which consists of 17 proteins associated with inflammation and correlated with the 10-year risk of end-stage renal disease in diabetic kidney disease. Multiple ongoing clinical trials explore the potential of proteomics and metabolomics in nephrology, aiming to validate novel biomarkers that provide clinically relevant information for early diagnosis and personalized treatment decisions. Additionally, autoantibodies in membranous nephropathy and biomarkers for acute kidney injury show promise in improving diagnosis and management. The field of nephrology biomarkers is rapidly evolving, offering potential advancements in early detection, disease progression prediction, and therapeutic interventions.
RNA biomarkers
MicroRNAs (miRNA) are stable molecules and there are several examples of their potential use in the context of kidney injury, including drug-induced kidney injury (DIKI). A cross-laboratory program to identify urinary miRNA patterns associated with cell- or cause-specific DIKI characterized biomarkers of glomerular, proximal tubule, thick ascending limb (TAL) of the loop of Henle or collecting duct (CD) injury in rats by exposing them to cell-specific toxins and confirming the location of increased expression by laser capture microdissection of nephron segments. Urinary miR-192-5p was identified as potentially proximal tubule-specific. Urinary miR-221-3p, miR-222-3p and miR-210-3p increased following exposure to TAL toxins, and miR-23a-3p following the podocyte toxin doxorubicin. Thus, urinary miRNA panels from different nephron regions may contribute to the exploring the DIKI potential of novel drugs.
Cell-free DNA
Cell-free DNA methods have increasingly been used, along with other methods, especially in the field of hematology and oncology to detect malignancies and evaluate recurrences. Similarly, they have potential for use in the detection of renal cell carcinoma. though it is too early to draw conclusions, there is potential for cell-free DNA to be used in the detection of acute rejection in kidney transplant recipients. Additionally, high levels of cell-free DNA were associated with adverse outcomes in one study of 131 CKD patients not on dialysis and in another study conducted on 289 patients on hemodialysis. Additionally, cell-free DNA was associated with AKI after cardiac surgery or in patients with type 1 cardiorenal syndrome. However, these data should be validated in large scale multicenter clinical studies that address the added benefit on patient management of assessing cell-free DNA.
Novel therapeutic alternatives
Novel therapeutic alternatives for ESRD include wearable artificial kidneys, xenotransplantation, stem cell–based therapy, and bioengineered and bio-artificial kidneys. Of note, one of the main objectives of these novel therapeutic approaches should be to maintain patients at home and to avoid dialysis centers. Additionally, novel medications to prevent CKD progression or treat CKD complications are at advanced stages of clinical development or have already been approved for clinical use in some countries.
Medications on the rise
Nonsteroidal MRA
Finerenone, a non-steroidal selective mineralocorticoid receptor antagonist, has shown promise in protecting the kidneys and cardiovascular system in patients with diabetic kidney disease. It improves cardiovascular outcomes, reduces the risk of CKD progression, and is approved for the treatment of CKD with albuminuria. Other non-steroidal selective MRAs are also being investigated. Aldosterone synthase inhibitors, which target aldosterone production, have potential in treating heart failure, hypertension, and kidney diseases, but further trials are needed to understand their clinical effects.
Endothelin receptor antagonists
Endothelin receptor antagonists (ERAs) have shown kidney protective effects in chronic kidney disease (CKD) and proteinuria, but they are associated with sodium retention and volume overload as a safety concern. Older ERA drugs like bosentan and atrasentan demonstrated some kidney protection in CKD patients, but a pivotal trial of atrasentan for diabetic kidney disease was terminated due to insufficient cardiovascular protection. Sparsentan, which acts as both an endothelin receptor-A inhibitor and an angiotensin receptor blocker, was superior to irbesartan in reducing proteinuria without adverse effects. Other ERAs like sitaxentan and zibotentan have also shown positive effects on kidney disease. Co-administration of ERAs with sodium-glucose cotransporter 2 (SGLT2) inhibitors may improve the safety profile and enhance kidney protection, and ongoing clinical trials are investigating this combination therapy. Selective ERA-A blockers are being explored as a potential future option to address the sodium retention issue.
HIF stabilizers
HIF prolyl hydroxylase inhibitors, or HIF stabilizers, are oral agents used to treat anemia associated with chronic kidney disease (CKD). They offer the advantage of oral administration compared to subcutaneous injections of erythropoietin (EPO) analogs. While some HIF stabilizers are in clinical use in China and Japan, roxadustat was recently approved by the European Medicines Agency (EMA). However, the U.S. Food and Drug Administration (FDA) recently rejected roxadustat and vadadustat due to safety concerns. The cardiovascular safety of HIF stabilizers remains inconclusive, and their effect on preserving kidney function is unclear. Recent studies have shown varied cardiovascular safety outcomes depending on the population and type of HIF stabilizer being used. Further large-scale studies are needed to investigate the efficacy and safety of HIF stabilizers in different populations.
Voclosporin
In a phase 3 clinical trial, voclosporin, a novel calcineurin inhibitor, demonstrated better kidney outcomes in patients with active lupus nephritis compared to placebo. The trial included 357 subjects who received voclosporin alongside mycophenolate mofetil (MMF) and low-dose corticosteroids. Voclosporin improved measures such as urine protein to creatinine ratio and estimated glomerular filtration rate (eGFR) without additional adverse effects. Another clinical trial confirmed the superior kidney outcomes of voclosporin in both low and high dose groups compared to placebo, but also noted a higher risk of adverse events, including deaths. Despite the higher risk of deaths in the low-dose group, voclosporin was recently approved by the FDA as the first drug for active lupus nephritis.
Conclusion
In summary, advancements in various aspects of kidney disease are expected to lead to earlier detection, more effective interventions, improved kidney replacement therapies, and better management of complications. To achieve this, it is important to define target groups and identify patients who would benefit the most from these advancements. Diagnostic markers have the potential to enable early detection of kidney disease, while novel therapies could slow its progression and reduce complications, potentially avoiding the need for kidney transplantation or renal replacement therapy. However, large-scale clinical studies with reliable outcomes are necessary before these therapeutic and diagnostic modalities can be widely used, making it challenging to provide a specific timeline for these developments.
References:
1. Jager KJ, Kovesdy C, Langham R et al. A single number for advocacy and communication-worldwide more than 850 million individuals have kidney diseases. Nephrol Dial Transplant 2019;34:1803–5. http://dx.doi.org/10.1093/ndt/gfz174.
2. Johansen KL, Chertow GM, Foley RN et al. US Renal Data System 2020 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis 2021;77:A7–8. http://dx.doi.org/10.1053/j.ajkd.2021.01.002.
3. Kramer A, Pippias M, Noordzij M et al. The European Renal Association – European Dialysis and Transplant Association (ERA-EDTA) registry annual report 2015: a summary. Clin Kidney J 2018;11:108–22. http://dx.doi.org/10.1093/ckj/sfx149.
4. Heaf J. Current trends in European renal epidemiology. Clin Kidney J 2017;10:149–53. http://dx.doi.org/10.1093/ckj/sfw150.
5. Hart A, Lentine KL, Smith JM et al. OPTN/SRTR 2019 annual data report: kidney. Am J Transplant 2021;21 Suppl 2:21–137. http://dx.doi.org/10.1111/ajt. 16502.
6. Ortiz A, Asociación Información Enfermedades Renales Genéticas (AIRG-E), European Kidney Patients’ Federation (EKPF) et al. RICORS2040: the need for collaborative research in chronic kidney disease. Clin Kidney J 2022;15:372–87. http://dx.doi.org/10.1093/ckj/sfab170.
7. Mehrotra R, Devuyst O, Davies SJ et al. The current state of peritoneal dialysis. J Am Soc Nephrol 2016;27:3238–52. http://dx.doi.org/10.1681/ASN.2016010112.
8. Perez-Gomez MV, Bartsch LA, Castillo-Rodriguez E et al. Clarifying the concept of chronic kidney disease for non-nephrologists. Clin Kidney J 2019;12:258–61. http://dx.doi.org/10.1093/ckj/sfz007.
9. Fernandez-Fernandez B, Sarafidis P, Kanbay M et al. SGLT2 inhibitors for non-diabetic kidney disease: drugs to treat CKD that also improve glycaemia. Clin Kidney J 2020;13:728–33. http://dx.doi.org/10.1093/ckj/sfaa198.
10. Gorostidi M, Sanchez-Martinez M, Ruilope LM et al. Chronic kidney disease in Spain: prevalence and impact of accumulation of cardiovascular risk factors. Nefrologia (Engl Ed) 2018;38:606–15. http://dx.doi.org/10.1016/j.nefroe.2018.04.010.
11. Ruilope LM, Ruiz-Hurtado G, Miranda B et al. Use of chronic kidney disease blind spot to prevent cardiorenal outcomes. Eur Heart J 2022;43:257–60. http://dx.- doi.org/10.1093/eurheartj/ehab456.
12. Sanchez-Nino MD, Sanz AB, Ramos AM et al. Clinical proteomics in kidney disease as an exponential technology: heading towards the disruptive phase. Clin Kidney J 2017;10:188–91. http://dx.doi.org/10.1093/ckj/sfx023.
13. Sanchez-Nino MD, Fernandez-Fernandez B, Ortiz A. Klotho, the elusive kidney-derived anti-ageing factor. Clin Kidney J 2020;13:125–7. http://dx.- doi.org/10.1093/ckj/sfz125.
14. Bennett KM, Baldelomar EJ, Charlton JR. Delivering on the potential of measuring nephron number in the clinic. Nat Rev Nephrol 2022;18:271–2. http://dx.- doi.org/10.1038/s41581-022-00560-5.
15. Luyckx VA, Rule AD, Tuttle KR et al. Nephron overload as a therapeutic target to maximize kidney lifespan. Nat Rev Nephrol 2022;18:171–83. http://dx.- doi.org/10.1038/s41581-021-00510-7.
16. Baldelomar EJ, Charlton JR, Beeman SC et al. Measuring rat kidney glomerular number and size in vivo with MRI. Am J Physiol Renal Physiol 2018;314:F399–f406. http://dx.doi.org/10.1152/ajprenal.00399.2017.
17. Puelles VG, Combes AN, Bertram JF. Clearly imaging and quantifying the kidney in 3D. Kidney Int 2021;100:780–6. http://dxdoi.org/10.1016/j.kint.2021.
18. Xie L, Koukos G, Barck K et al. Micro-CT imaging and structural analysis of glomeruli in a model of adriamycin-induced nephropathy. Am J Physiol Renal Physiol 2019;316:F76–89. http://dx.doi.org/10.1152/ajprenal.00331.2018.