Introduction
It’s not unusual to receive a cancer diagnosis along with a pericardial effusion. The primary cause of pericardial effusion in myeloproliferative diseases and other cancers is the direct invasion of tumour into the pericardium. Pericardial effusion, however, seems to be immune-mediated or treatment-related in myelodysplastic syndrome (MDS). In addition, bone marrow suppression in MDS patients causes immunosuppression, which can result in infectious pericardial effusions. Radiation therapy, disease-modifying immunotherapies (such as alemtuzumab and immune checkpoint inhibitors), and several types of chemotherapeutic drugs (such as azacitidine, cytarabine, fludarabine, doxorubicin, docetaxel, and dasatinib) can all result in pericardial illness with effusion. Additionally, it has been proposed that autoimmune processes linked to cancer can result in an inflammatory effusion in patients who have neither infection nor direct cancer invasion. Nevertheless, only one published case report describes a pericardial effusion attributable to immune thrombocytopenia (ITP), making pericardial effusions related to hematologic disorders incredibly rare. This article describes a case study of pericardial effusion in a middle-aged man who had pancytopenia.
Case Study
A male in his late 50s with a history of type 2 diabetes mellitus, hypertension, hyperlipidemia, gout, and stage 3A chronic kidney disease presented with a five-month history of progressive shortness of breath, fatigue, and lower extremity edema. A trial of furosemide by his primary care physician did not alleviate his symptoms, after which a complete blood count (CBC) showed marked pancytopenia, specifically moderate macrocytic anemia (hemoglobin of 8.6 g/dl), mild neutropenia (white blood cell count of 3,400/µl), and severe thrombocytopenia (platelet count of 1,600/µl). A computed tomography (CT) scan of the chest showed some borderline lymph nodes, and a CT scan of the abdomen/pelvis showed mesenteric lymphadenopathy, but these findings resolved on subsequent imaging. As such, bone marrow biopsy was performed and demonstrated the absence of platelet-making megakaryocytes with no overt dyspoiesis in granulocytes and erythroid precursors, normal marrow cellularity (1-2:1 fat-to-cell ratio), and normal iron stores. These findings, specifically the amegakaryocytic thrombocytopenia in conjunction with normal cellularity, did not fully explain the blood counts, which raised the question of occult chronic immune thrombocytopenia (ITP) versus MDS. Due to the severity of the patient’s symptoms and pancytopenia, a biopsy was repeated to rule out MDS but showed similar results. At this time, the patient was noted to have a large pericardial effusion, which was drained. Unfortunately, his pancytopenia progressed with a hemoglobin of 5.2 g/dl from 9.6 g/dl, leukopenia of 1,800/μl from 5,100/μl, and rapid severe thrombocytopenia; one CBC showed a platelet count of 0/μl from 3,000/μl. At that point, he was transferred to a tertiary care center for further workup. A subsequent third biopsy performed 4-5 months after the initial biopsies showed 5% cellularity with decreased trilineage hematopoiesis (Figure 1).
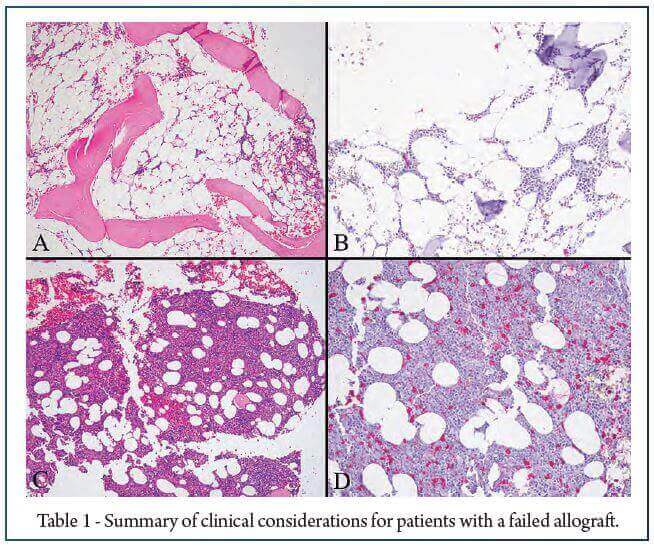
Thus, the findings were felt to be most consistent with severe aplastic anemia (SAA).Interestingly, a small, asymptomatic pericardial effusion had reaccumulated one month after his discharge. With the recurrence of the pericardial effusion, the decision was made to proceed with a subxiphoid pericardial window due to the posterior placement of the effusion. Post-procedure echocardiography performed two months later showed a smaller pericardial effusion without signs of valvular dysfunction or hemodynamic compromise. Due to pancytopenia secondary to SAA and the presence of bleeding hemorrhoids on readmission, the patient received frequent platelet transfusions and one packed red blood cell transfusion to maintain his platelets above 20,000/µl and hematocrit above 20%. Unfortunately, the patient became transfusion-dependent, and bone marrow transplantation (BMT) was persistently delayed by infectious complications. During pretransplant evaluation, the patient was found to have monosomy 7 MDS by bone marrow biopsy rendering him ineligible for BMT. This was supported by the development of recurrent, bilateral, sanguineous pleural effusions, which initially showed reactive mesothelial cells but subsequently exhibited abnormal myeloblasts with aberrant expression of cluster of differentiation 7 (CD7) and cluster of differentiation 56 (CD56) by flow cytometry, concerning for conversion of MDS to acute leukemia. He died three days later prior to follow-up. Of note, he was profoundly immunosuppressed and had pancytopenia immediately prior to his death with WBCs of 1,700/µl, absolute neutrophil count (ANC) of 650/µl, hemoglobin of 7.3 g/dl, and platelet count of 78,000/µl.
Conclusions
Pericardial effusions are characterized by the accumulation of greater than 50 mL of fluid between the visceral and parietal pericardium. They are a commonly encountered finding in clinical practice but not always associated with concomitant pericarditis. The differential diagnosis is broad but can be simply classified as infectious or non-infectious with non-infectious causes being further subclassified as neoplastic, traumatic, metabolic, immunologic, or idiopathic. Despite this broad differential, in most cases of pericardial effusion, particularly small pericardial effusions, no etiology is found. In this report, we describe a case of aplastic anemia that presented with a large inflammatory pericardial effusion in the absence of pericarditis and posit a shared autoimmune phenomenon as a potential explanation for the finding. Furthermore, several therapies used in hematologic malignancies can cause pericardial effusions, but two to consider are as follows: (1) immunosuppressive drugs used for SAA or in the setting of hematopoietic stem cell transplant (i.e., cyclosporine, sirolimus, and alemtuzumab) and (2) alkylating/hypomethylating cytotoxic agents used for myeloid malignancies (i.e., azacytidine, cytarabine, cyclophosphamide, and fludarabine).
References:
1. Choi JH, Ahn MJ, Park YW, Oh HS, Lee YY, Kim IS: A case of erythema nodosum and serositis associated with myelodysplastic syndrome. Korean J Intern Med. 2005, 20:177-9. 10.3904/kjim.2005.20.2.177.
2. Fernández-Sojo J, Vives S, Oliveras Vilà T, Ribera JM: [Exudative pericardial effusion and oligoarthritis in a patient newly diagnosed with myelodysplastic syndrome] (Article in Spanish). Med Clin (Barc). 2014, 143:43-4. 10.1016/j.medcli.2013.09.009.
3. Goo K, Uy R, Roswarski J: Azacitidine-associated pleuropericardial effusion in myelodysplastic syndrome: a case report. J Oncol Pharm Pract. 2019, 25:1248-52. 10.1177/1078155218784762.
4. Fogaça da Mata M, Vieira Martins M, Rato J, Madeira M, Gonçalves JP, Teixeira A, Anjos R: Azacitidine-induced massive pericardial effusion in a child with myelodysplastic syndrome. J Oncol Pharm Pract. 2022, 28:975-8. 10.1177/10781552211073884.
5. Brook I: Pericarditis due to anaerobic bacteria. Cardiology. 2002, 97:55-8. 10.1159/000057672.
6. Chahine J, Shekhar S, Mahalwar G, Imazio M, Collier P, Klein A: Pericardial involvement in cancer. Am J Cardiol. 2021, 145:151-9. 10.1016/j.amjcard.2020.12.092.
7. Azarbal A, LeWinter MM: Pericardial effusion. Cardiol Clin. 2017, 35:515-24. 10.1016/j.ccl.2017.07.005.
8. Jain S, Singh P, Naidu S, Sharma A: Cyclosporine-induced pericarditis: an elusive cause of chest pain in Behçet’s disease. BMJ Case Rep. 2019, 12:e229433. 10.1136/bcr-2019-229433.
9. Alroughani R, Van Wijmeersch B, Al Khaboori J, et al.: The use of alemtuzumab in patients with relapsing-remitting multiple sclerosis: the Gulf perspective. Ther Adv Neurol Disord. 2020, 13:1756286420954119. 10.1177/1756286420954119.
10. Levy PY, Corey R, Berger P, et al.: Etiologic diagnosis of 204 pericardial effusions. Medicine (Baltimore). 2003, 82:385-91. 10.1097/01.md.0000101574.54295.73.
11. Ma W, Liu J, Zeng Y, et al.: Causes of moderate to large pericardial effusion requiring pericardiocentesis in 140 Han Chinese patients. Herz. 2012, 37:183-7. 10.1007/s00059-011-3428-5.
12. Peña-Garcia JI, Shaikh SJ, Villacis-Nunez DS, Gurram MK: Pericardial effusion in systemic sarcoidosis: a rare manifestation of cardiac sarcoid. Heart Views. 2019, 20:56-9. 10.4103/HEARTVIEWS.HEARTVIEWS_117_18.