Introduction
Ocular graft-versus-host-disease (GVHD) remains a significant clinical complication after allogeneic hematopoietic stem cell transplantation. Impaired visual function, pain, and other symptoms severely affect affected individuals’ quality of life. However, the diagnosis of and therapy for ocular GVHD involve a multidisciplinary approach and remain challenging for both hematologists and ophthalmologists, as there are no unified international criteria. Through an exploration of the complex pathogenesis of ocular GVHD, this review comprehensively summarizes the pathogenic mechanism, related tear biomarkers, and clinical characteristics of this disease. Novel therapies based on the mechanisms are also discussed to provide insights into the ocular GVHD treatment.
Pathogenic mechanism and novel therapeutic targets
Lacrimal gland hypofunction
Ocular graft-versus-host disease (GVHD) primarily affects the lacrimal gland (LG) in the eye. Donor T cells infiltrate the LG and cause tissue damage, leading to inflammation and the recruitment of immune cells.

CD34+ fibroblasts are also recruited and activated, contributing to excessive collagen assembly and inflammation. Senescent cells and oxidative stress play a role in the pathogenesis of ocular GVHD. These changes result in fibrosis and decreased tear production. Further research is needed to understand the relationship between specific molecules and the development of ocular GVHD.
Corneal impairment
Ocular graft-versus-host disease (GVHD) can lead to complications in the cornea, causing symptoms such as pain, photophobia, and vision impairment. Corneal epithelial damage, including punctate keratopathy and persistent defects, is common. Severe cases can result in corneal ulceration, neovascularization, and limbal stem cell deficiency. Inflammation in ocular GVHD affects all layers of the cornea, including the endothelium, leading to a decrease in endothelial cell density. The activation of the SP/NK1R pathway and the release of pro-inflammatory cytokines contribute to corneal endothelial cell loss. Corneal neurosensory abnormalities may also occur. Further research is needed to understand the underlying mechanisms and develop effective treatments for these corneal complications.
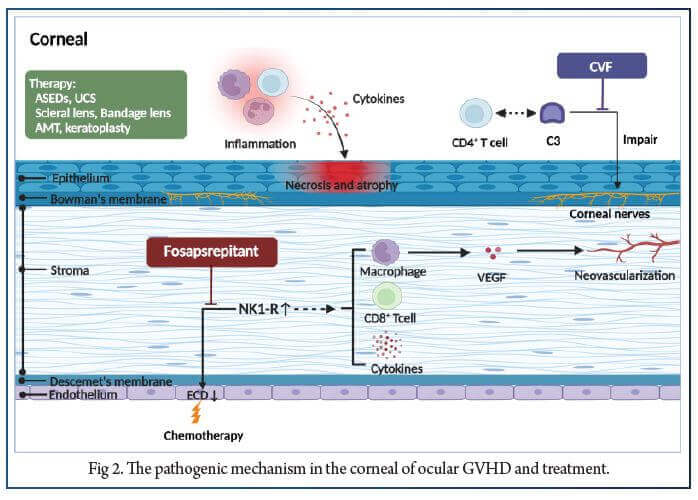
Autologous serum eye drops (ASEDs) containing wound healing factors have shown effectiveness in treating severe cases of ocular GVHD. However, concerns remain regarding infection risk, long-term application side effects, and availability for certain patients. Alternative options include allogeneic serum, umbilical cord serum, and platelet-derived eye drops, but caution is necessary to avoid complications. Scleral lenses, bandage soft contact lenses, amniotic membrane grafts, and surgical procedures like limbal epithelial transplantation and keratoplasty are potential treatments for refractory ocular surface and severe keratitis sicca in ocular GVHD. Inhibition of the SP-NK1R axis with fosaprepitant has shown promise in reducing corneal staining and inflammation in ocular GVHD. Additionally, localized cobra venom factor (CVF) treatment has prevented corneal sensation loss in animal models of ocular GVHD. However, further research is needed to evaluate the therapeutic potential of CVF in human patients.
Conjunctival involvement
Conjunctival involvement in ocular GVHD is characterized by lymphocytic infiltration, fibrosis, and altered mucosal microvilli. Complications can include cicatricial conjunctivitis, entropion, symblepharon, ankyloblepharon, and lagophthalmos. Superior limbal keratoconjunctivitis (SLK) is a recently reported manifestation. Topical steroids, calcineurin inhibitors (such as cyclosporine A and tacrolimus), and NET-dismantling biologics show promise in managing ocular GVHD. Autologous serum eye drops and blood-derived products are alternative therapeutic options. The microbiome and oral antibiotics are also being explored for systemic GVHD treatment. Further research is needed to understand these treatment approaches fully.
Meibomian gland dysfunction
Meibomian gland dysfunction (MGD) is a common complication of ocular GVHD, characterized by morphological and functional alterations in the meibomian glands. MGD in ocular GVHD is associated with ductal epithelial hyperkeratinization, lymphocyte infiltration, and fibrosis. These changes result in abnormal lipid secretion, tear film instability, and ocular surface damage. Eyelid margin abnormalities further contribute to ocular discomfort. Treatment options for MGD in ocular GVHD include warm compresses, lid hygiene, antibiotic ointments, and nutritional supplements. In severe cases, partial tarsorrhaphy may be considered to protect the cornea. Further research is needed to better understand the pathogenesis and develop effective interventions for MGD in ocular GVHD.
Other new therapies
Several novel treatments for ocular GVHD show promise in reducing inflammation and improving clinical outcomes. In preclinical models, inhibitors of vascular adhesion protein-1 and CCR ligand 21, as well as gene transfer therapy using AAV-HLA-G, have shown efficacy in reducing inflammation. Inhibitors of Janus kinase (JAK) and spleen tyrosine kinase (SYK), such as ruxolitinib and combined JAK/SYK inhibitors, have demonstrated improvement in ocular GVHD symptoms. Cell-based therapies, including mesenchymal stromal cells (MSCs) and regulatory T cells (Tregs), have shown potential in reducing inflammation and improving ocular symptoms. Topical medications like rebamipide, diquafosol, and lifitegrast have also shown efficacy in improving clinical signs and symptoms. Several ongoing clinical trials are evaluating additional novel therapeutics for ocular GVHD.
Ocular GVHD biomarkers
Cellular mediators, such as tear cytokines/chemokines, lipid metabolites, and proteins, have been identified as potential biomarkers for ocular GVHD. These biomarkers can aid in diagnosis, prediction, prognosis, and monitoring of the disease. Various cytokines, including IL-1, IL-2, IL-6, IL-8, IL-10, IL-17, IP-10/CXCL-10, ICAM-1, TNF- , EGF, and LT- , have been associated with ocular GVHD and can serve as biomarkers. Tear protein profiling has identified differentially expressed proteins, such as histone H2B and lactotransferrin, that may be potential biomarkers. Lipid metabolic pathways have also shown dysregulation in ocular GVHD, with elevated levels of phosphatidylcholines, serine, sphingomyelin, lactosylceramide, and certain fatty acids. These lipid metabolites could serve as diagnostic biomarkers and therapeutic targets. Additionally, cellular components such as neutrophils, exfoliated epithelial cells, and NET-associated proteins have shown potential as biomarkers for ocular GVHD.
Conclusion
Ocular GVHD is a challenging condition to diagnose and treat, leading to a significant impact on patients’ quality of life. Early diagnosis and intervention are crucial to prevent irreversible damage to the ocular tissues. New diagnostic methods, including ocular surface biomarkers, can aid in early detection and monitoring treatment response. Prevention and regular follow-up are essential for better management of ocular GVHD. Further research on the underlying mechanisms will help develop targeted treatments for improved outcomes in patients with ocular GVHD.
References:
1. Zhang X, Chen J, Han M-Z, Huang H, Jiang E, Jiang M, et al.. The consensus from the Chinese society of hematology on indications, conditioning regimens and donor selection for allogeneic hematopoietic stem cell transplantation: 2021 update. J Hematol OncolJ Hematol Oncol (2021) 14:145. doi: 10.1186/s13045-021-01159-2.
2. Wang X, Huang R, Zhang X, Zhang X. Current status and prospects of hematopoietic stem cell transplantation in China. Chin Med J (Engl) (2022) 135:1394–403. doi: 10.1097/CM9.0000000000002235.
3. Jagasia MH, Greinix HT, Arora M, Williams KM, Wolff D, Cowen EW, et al.. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-Host disease: I. the 2014 diagnosis and staging working group report. Biol Blood Marrow Transpl (2015) 21:389–401.e1. doi: 10.1016/j.bbmt. 2014.12.001.
4. Pathak M, Diep PP, Lai X, Brinch L, Ruud E, Drolsum L. Ocular findings and ocular graft-versus-host disease after allogeneic stem cell transplantation without total body irradiation. Bone Marrow Transpl (2018) 53:863–72. doi: 10.1038/s41409-018-0090-z.
5. Sarbay H, Hagverdiyeva S, Turkkan E, Akcay S, Atay A, Malbora B. Ophthalmologic findings and complications before and after hematopoietic stem cell transplantation: single-center study. Int Ophthalmol (2021) 41:2533–8. doi: 10.1007/s10792-021-01811-3.
6. Qiu Y, Hong J, Peng R. Manifestation of clinical categories of ocular graft-versus-Host disease. J Ophthalmol (2018) 2018:1–7. doi: 10.1155/2018/6430953 [PMC free article].
7. Ogawa Y, Kim SK, Dana R, Clayton J, Jain S, Rosenblatt MI, et al.. International chronic ocular graft-vs-Host-Disease (GVHD) consensus group: proposed diagnostic criteria for chronic GVHD (Part I). Sci Rep (2013) 3:3419. doi: 10.1038/srep03419.
8. Ogawa Y, Okamoto S, Wakui M, Watanabe R, Yamada M, Yoshino M, et al.. Dry eye after haematopoietic stem cell transplantation. Br J Ophthalmol (1999) 83:1125–30. doi: 10.1136/bjo.83.10.1125.
9. Wolff D, Radojcic V, Lafyatis R, Cinar R, Rosenstein RK, Cowen EW, et al.. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-Host disease: IV. the 2020 highly morbid forms report. Transpl Cell Ther (2021) 27:817–35. doi: 10.1016/j.jtct.2021.06.001.
10. Giannaccare G, Pellegrini M, Bernabei F, Scorcia V, Campos E. Ocular surface system alterations in ocular graft-versus-host disease: all the pieces of the complex puzzle. Graefes Arch Clin Exp Ophthalmol (2019) 257:1341–51. doi: 10.1007/s00417-019-04301-6.