Introduction
(Article introduction authored by Conquest Editorial Team)
Acquired aplastic anemia (AA) in children is a rare and life-threatening bone marrow failure disorder, distinct in its diagnosis and treatment from adult AA.
Accurate diagnosis is critical, requiring differentiation from refractory cytopenia of childhood and inherited bone marrow failure syndromes through detailed morphological evaluation and genetic analysis using next-generation sequencing. Treatment considerations must also account for long-term sequelae and impacts on daily life.
Immunosuppressive therapy (IST) and hematopoietic cell transplantation (HCT) have improved survival rates to 90%. Recent advancements in HCT, including improved conditioning regimens and the successful use of matched unrelated donor (MUD) transplants, unrelated cord blood transplants, and haploidentical HCT, have significantly enhanced outcomes for pediatric AA patients. This review covers the latest advances in diagnosis and treatment, providing an updated algorithm for managing pediatric acquired AA.
Differential diagnosis of pediatric acquired AA
RCC
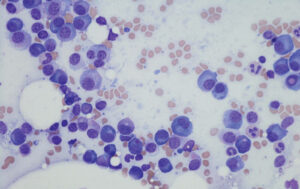
Diagnosing bone marrow failures (BMFs) in children is challenging, particularly distinguishing between aplastic anemia (AA) and hypoplastic myelodysplastic syndromes (MDS), especially refractory cytopenia of childhood (RCC). RCC, a provisional entity in the WHO classification of childhood MDS, often presents with hypoplastic bone marrow (BM) and is commonly treated as AA.
Both BM biopsy and aspiration are crucial for assessing BM cellularity due to its patchy nature. (Fig. 1) Despite controversies over RCC’s classification, a Japanese study found no differences in response to immunosuppressive therapy (IST), clonal evolution, or overall survival (OS) among children with AA, RCC without multilineage dysplasia (MLD), and RCC with MLD. Thus, AA and hypoplastic RCC require similar clinical care and treatment.
Diagnostic approach incorporating comprehensive genetic testing
Differentiating inherited bone marrow failure syndromes (IBMFS) from acquired aplastic anemia (AA) is crucial for effective treatment. Treating IBMFS as AA can lead to poor response to immunosuppressive therapy (IST) and increased toxicity during hematopoietic cell transplantation (HCT). IBMFS, which accounts for 10-20% of pediatric BMF cases, can also affect adolescents and young adults.
Diagnosis is complicated by cryptic or atypical presentations, necessitating comprehensive diagnostic work-ups, including family history, physical exams, blood and bone marrow evaluations, and genetic analyses like next-generation sequencing (NGS). A recent US study found that 6.6% of patients clinically diagnosed with acquired AA actually had IBMFS, which was associated with inferior survival due to treatment-related mortality.

Conditioning regimens for acquired BMF in children
Bone marrow transplantation (BMT) is a well-established treatment for pediatric acquired bone marrow failure (BMF), such as aplastic anemia (AA), achieving a 90% survival rate.
The traditional conditioning regimen of cyclophosphamide (CY) and antithymocyte globulin (ATG) has been modified due to CY’s toxicity, incorporating fludarabine (FLU) to reduce CY dosage.
The European Group for Blood and Marrow Transplantation (EBMT) recommends a regimen of FLU, lower-dose CY (1200 mg/m2), and ATG for pediatric patients, and the same regimen with 2 Gy total body irradiation (TBI) for adults. However, graft failure, especially late graft failure (LGF), remains a concern.
A prospective US study recommended CY doses of 50-100 mg/kg to reduce graft failure rates, but LGF incidence remained high at 12-15%. An alternative approach incorporating other alkylating agents, like melphalan (MEL), showed promising results.
A Japanese study involving 367 children with acquired BMF demonstrated that a FLU/MEL-based regimen resulted in 98% overall survival (OS) and 97% failure-free survival (FFS), with a reduced LGF incidence of 3% and no donor-type aplasia.
Consequently, a regimen of FLU, MEL (140 mg/m2), and ATG, with or without low-dose TBI, has been adopted in Japan’s treatment guidelines for pediatric BMF to prevent complications and avoid re-transplantation.
Upfront unrelated donor BMT
In children with acquired aplastic anemia (AA), bone marrow transplantation (BMT) from a matched related donor (MRD) has been the preferred treatment. Recently, donors have been expanded to include one-locus mismatched related donors (1MMRD).
For patients lacking an MRD, immunosuppressive therapy (IST) with antithymocyte globulin (ATG) and cyclosporine (CyA) has been the first-line therapy, with BMT from a matched unrelated donor (MUD) as a salvage option for IST non-responders.
However, recent improvements have made upfront MUD BMT a viable first-line option.
A UK study showed excellent outcomes for upfront MUD BMT in patients under 20, with a 2-year overall survival (OS) and failure-free survival (FFS) of 96% and 92%, respectively.
An EBMT study reported promising results for upfront MUD BMT, with a 2-year OS and GVHD-free/relapse-free survival (GRFS) of 89% and 86%, respectively, particularly favorable for children under 15 years, with a GRFS exceeding 90%.
Consequently, several guidelines now recommend upfront MUD BMT for children with acquired AA who lack an MRD, provided a MUD is available within 2-3 months of diagnosis.
Ongoing prospective trials aim to confirm this strategy as the standard of care, addressing limitations from previous retrospective studies.
Options for second-line treatment: UCBT and haploidentical HCT
Advances in supportive care, conditioning regimens, and novel GVHD prophylaxis have expanded treatment options for acquired AA patients without a matched BM donor, making UCBT and haploidentical HCT viable options.
Early UCBT studies showed high graft failure and low survival rates. However, recent improvements have significantly increased success rates.
A French study reported a 2-year OS rate of 81%, and a Japanese survey showed a 5-year OS rate of 100% in pediatric patients. Conditioning regimens without ATG have also shown better outcomes.
Haploidentical HCT, initially developed for hematological malignancies, has become a second-line treatment for AA. Innovations like ex vivo TCR-α/β-T cell depletion, in vivo T-cell depletion, and post-transplant CY have improved outcomes.
The PTCY approach demonstrated an 81% 1-year OS rate with no severe GVHD in a US trial, though graft failure remains a concern.
A Chinese study reported comparable long-term outcomes between haploidentical HCT and matched sibling donor HCT, with significant QOL improvements post-transplant.
These advances suggest that UCBT and haploidentical HCT are promising options for children with AA who lack a matched donor or in emergency situations.
Eltrombopag (EPAG) added to IST
Thrombopoietin receptor agonists like EPAG have recently shown efficacy in treating both refractory and untreated AA patients. In the RACE phase III trial by EBMT, adding EPAG to horse ATG and CyA improved the 6-month ORR from 41% to 68%.
However, a NIH study reported a high 4-year relapse rate of 43% among responders, despite an initial 81% ORR, and a 15% incidence of clonal evolution, comparable to conventional IST. For children, evidence on EPAG is limited.
The NIH study’s subgroup analysis found no improvement in the 6-month ORR for those under 18, with a higher relapse rate and lower 4-year FFS in the EPAG group. Additionally, 13% of these patients developed clonal evolution. A Russian study with 98 children also found no benefit in adding EPAG to IST.
Currently, there’s no evidence to support EPAG use in untreated pediatric AA, and its use should be cautious due to potential risks of clonal evolution.
Conclusion
As AA is rare in children, many pediatric hematologists have limited experience in its diagnosis and treatment. Children with BMF should be referred to specialized centers for comprehensive diagnostic work-ups, including genetic analysis using NGS. Guidelines from various countries now recommend incorporating genetic testing for pediatric AA diagnosis and treatment decisions.
The current treatment algorithm for pediatric AA involves BMT from a MRD or 1MMRD as the first choice, with MUD as a viable first-line option if available. UCBT and haploidentical HCT are promising for emergencies or when no matched donors are available.
The FLU/MEL-based regimen is becoming a standard for conditioning to overcome LGF, a major HCT complication. Long-term follow-up is crucial to detect treatment-related complications and assess QOL.
Future developments should focus on diagnosis, treatment, patient education, and the transition from pediatric to adult care.
1. Kojima S, Horibe K, Inaba J, Yoshimi A, Takahashi Y, Kudo K, et al. Long-term outcome of acquired aplastic anaemia in children: comparison between immunosuppressive therapy and bone marrow transplantation. Br J Haematol. 2000;111:321–8.
2. Yoshida N, Kobayashi R, Yabe H, Kosaka Y, Yagasaki H, Watanabe K, et al. First-line treatment for severe aplastic anemia in children: bone marrow transplantation from a matched family donor versus immunosuppressive therapy. Haematologica. 2014;99:1784–91.
3. Dufour C, Pillon M, Socie G, Rovo A, Carraro E, Bacigalupo A, et al. Outcome of aplastic anaemia in children. A study by the severe aplastic anaemia and paediatric disease working parties of the European group blood and bone marrow transplant. Br J Haematol. 2015;169:565–73.
4. Atmar K, Ruivenkamp CAL, Hooimeijer L, Nibbeling EAR, Eckhardt CL, Huisman EJ, et al. Diagnostic value of a protocolized in-depth evaluation of pediatric bone marrow failure: a multi-center prospective cohort study. Front Immunol. 2022;13: 883826.
5. Keel S, Geddis A. The clinical and laboratory evaluation of patients with suspected hypocellular marrow failure. Hematol Am Soc Hematol Educ Program. 2021;1:134–42.
6. Shimano KA, Narla A, Rose MJ, Gloude NJ, Allen SW, Bergstrom K, et al. Diagnostic work-up for severe aplastic anemia in children: consensus of the North American pediatric aplastic anemia consortium. Am J Hematol. 2021;96:1491–504.
7. Muramatsu H, Okuno Y, Yoshida K, Shiraishi Y, Doisaki S, Narita A, et al. Clinical utility of next-generation sequencing for inherited bone marrow failure syndromes. Genet Med. 2017;19:796–802.
8. Ohara A, Kojima S, Hamajima N, Tsuchida M, Imashuku S, Ohta S, et al. Myelodysplastic syndrome and acute myelogenous leukemia as a late clonal complication in children with acquired aplastic anemia. Blood. 1997;90:1009–13.
9. Socie G, Henry-Amar M, Bacigalupo A, Hows J, Tichelli A, Ljungman P, et al. Malignant tumors occurring after treatment of aplastic anemia. European bone marrow transplantation-severe aplastic anaemia working party. N Engl J Med. 1993;329:1152–7.
10. Yoshida N, Yagasaki H, Hama A, Takahashi Y, Kosaka Y, Kobayashi R, et al. Predicting response to immunosuppressive therapy in childhood aplastic anemia. Haematologica. 2011;96:771–4.
11. Narita A, Zhu X, Muramatsu H, Chen X, Guo Y, Yang W, et al. Prospective randomized trial comparing two doses of rabbit anti-thymocyte globulin in patients with severe aplastic anaemia. Br J Haematol. 2019;187:227–37.
12. Kikuchi A, Yabe H, Kato K, Koh K, Inagaki J, Sasahara Y, et al. Long-term outcome of childhood aplastic anemia patients who underwent allogeneic hematopoietic SCT from an HLA-matched sibling donor in Japan. Bone Marrow Transplant. 2013;48:657–60.
13. Vo P, Onstad L, Flowers ME, Storb R. Cancers after HLA-matched related bone marrow transplantation for aplastic anemia. Bone Marrow Transplant. 2022;57:83–8.
14. Yoshida N, Takahashi Y, Yabe H, Kobayashi R, Watanabe K, Kudo K, et al. Conditioning regimen for allogeneic bone marrow transplantation in children with acquired bone marrow failure: fludarabine/melphalan vs. fludarabine/cyclophosphamide. Bone Marrow Transplant. 2020;55:1272–81
You Might Also Like
Pericardial Effusion: A Novel Presentation of Aplastic Anemia

Cancers after hematopoietic cell transplantation for aplastic anemia—the importance of persistence