
Introduction
Precision medicine has already entered clinical practice in kidney transplantation. The individual degree of sensitization to alloimmune antigens is assessed by the detection of anti-HLA donor-specific antibodies in the donor and recipient human leucocyte antigen (HLA) regions, which are genotyped in two class 1 and frequently three class 2 loci. Non-HLA mismatches have recently been linked to outcomes like acute T- and B-cell-mediated rejection, as well as long-term graft survival.
Next-generation sequencing can be used to track particular alloimmune T- and B-cell clones, and it can also be used to refine the immunogenicity of allo-epitopes in their interactions with HLA and T- and B-cell receptors. Hemodialysis therapy prescription is far from accurate, in contrast to transplantation.The concept of ‘appropriate’ therapy based on urea elimination has been a key roadblock so far. Kt/Vurea and associated metrics do not indicate long-term results or the severity of uremic symptoms.
Other solutes responsible for particular aspects of uremic disease may now be indented using modern technology, and measuring them will be a vital step in going beyond the conventional prescription of hemodialysis.
The cohort approach to kidney transplantation
The success of kidney transplantation depends on histocompatibility. Before solid-phase technologies became widely available to determine the degree and specificity of allosensitization, the selection of a suitable donor kidney was based on low resolution human leucocyte antigen (HLA) typing by serology and updated every other year. The discovery and wider utilization of calcineurin-inhibitor-based maintenance immunosuppression in the early 1990s led to a dramatic improvement in short-term outcomes, but long-term graft survival of patients beyond 1 year remained almost unchanged.
A key reason for these shortcomings was the lack of individual immunological risk stratification and individualized maintenance immunosuppressive therapy. The clinical management after transplantation has been rather standardized with regular determination of estimated glomerular filtration rate (eGFR) and measurement of blood trough levels of maintenance immunosuppressive drugs such as calcineurin inhibitors.
Surprisingly, with this crude cohort-based management algorithm and rather imprecise diagnostic tools, most patients nonetheless exhibited a median graft survival of 10 years. However, an annual graft attrition rate of 5% specifically for live donor kidneys in not acceptable. In the last decade, great research efforts were undertaken to better understand alloimmunity and to determine a patient’s individual rejection risk for a specific donor to recipient HLA match on the level of a high-resolution DNA sequencing.
Adding the individualized perspective: the presence and near future of precision medicine
As the HLA system is the most polymorphic and genetically variable region in human, donor to recipient matching remains always a compromise between waiting time and the availability of a ‘suitable’ deceased or live donor kidney. This high resolution of the genetic makeup of the polymorphic HLA regions of the donor and the recipient together with the identification of unacceptable antigens based on single beat donor-specific antibody (DSA) determination allows for a precise risk assessment before transplantation.
These patients are usually highly sensitized and it may be necessary to transplant across a HLA barrier if other solutions are not available. On the other hand, the HLA proteins are encoded only on a short stretch of 4 million bases on chromosome 6 and there is particularly good evidence that genome-wide donor to recipient incompatibilities outside the HLA regions plays a critical role in ‘chronic rejection’ caused by indirect allorecognition of donor epitopes.
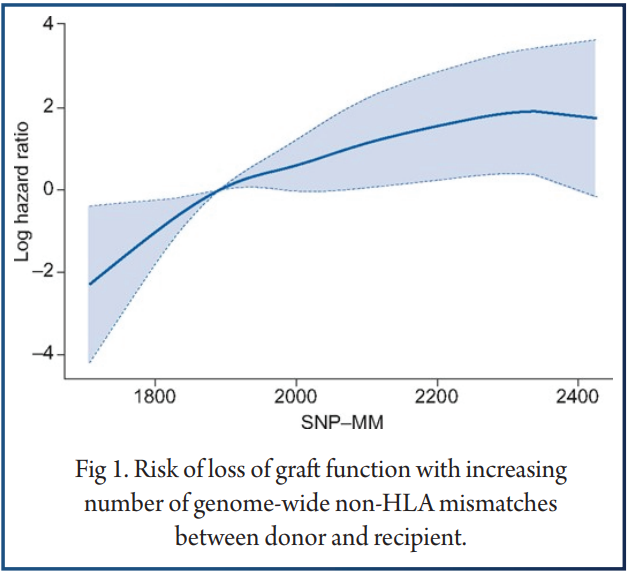
Reindl-Schwaighofer et al. showed that non-HLA incompatibilities of immune-accessible amino acid residues/peptides exhibit a similar threat to graft loss as HLA incompatibilities per unit increase of mismatches (Figure 1).
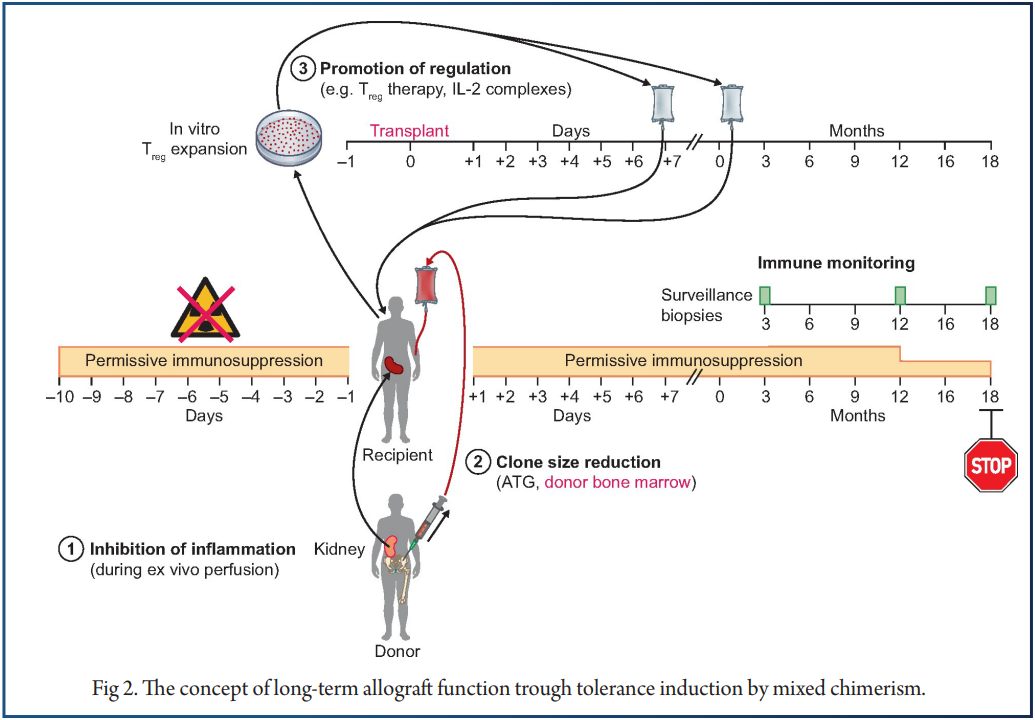
Given the complexity of the alloimmune response and considerable uncertainty on specific epitope immunodominance, a realistic strategy to improve long-term outcomes will be tolerance induction through mixed chimerism without toxic conditioning. In order to estimate the risk of a clinically relevant alloimmune response after transplantation, tracking of alloreactive T cells determined by mixed lymphocyte reaction has been suggested previously.
Persistence of DSAs after treatment of ABMR is likely caused by memory B cells and thus pre-transplant risk stratification based on the existence of alloimmune memory B cell may be feasible. Once the transplant has been performed, sequentially immune surveillance is performed in most transplant centers including DSA monitoring and management biopsies to guide individual immunosuppression. For example, almost half of the biopsies classified as ‘clean’ by pathologists show in fact molecular features of rejection (T-cell-mediated alloimmune response) and vice versa 50% of specimens classiffed as ABMR in histology were ‘clean’ molecularly. Treatment of acute T-cell-mediated rejection is usually successfully performed by high doses steroids or anti-thymocyte immunoglobulins.
Acute ABMR early after transplantation is also manageable but the treatment enigma persists for chronic ABMR.Promising preliminary data suggest that anti-interleukin-6 antibody treatment might be a good option for certain individuals, but the final proof will need larger studies. Based on these data, we conclude that precision diagnostics is already standard after kidney transplantation, but precision therapy is currently limited to risk-based pharmacodynamics of standard immunosuppressants (Figure 2)
Precision medicine in hemodialysis
Current shortcomings and barriers
While transplantation has advanced toward precision, hemodialysis has lagged far behind. This section will focus on our failure to adjust the hemodialytic removal of uremic solutes to the condition of individual patients, but we also offen fail to individualize hemodialysis treatment for control of calcium, potassium, acid–base and body fluid levels.Uniform prescription for all patients began early in the history of hemodialysis. This effort, which culminated in the United Sates National Cooperative Hemodialysis Study (NCDS), ended strangely as analysis showed that the fraction of urea removed during each of 3 weekly treatments, as reflected by Kt/Vurea, predicted outcomes better than the blood urea level.
Yet throughout the world today hemodialysis ‘adequacy’ is still commonly assessed by calculation of Kt/Vurea or a related urea kinetic parameter such as the equivalent renal urea clearance (EKR) or standard Kt/Vurea. So far, however, there has been little effort to develop chemical measures that better predict the effect of hemodialysis on either patients’ symptoms or their long-term outcomes. The tendency has been rather to prescribe a little more treatment than is necessary to meet urea kinetic targets, hoping that this will do the patients good. This is also apparent in guidelines for treatment duration.
The weakness of prescribing hemodialysis without regard to the differences among patients is even more clearly revealed in the treatment of patients with residual kidney function, the presence of which should lessen the requirement for hemodialysis. A well-reasoned case has been made for reducing the intensity of hemodialysis in patients with residual function and particularly in those initiating hemodialysis, yet many of these patients are prescribed treatment thrice weekly for a standard minimum time, even though there is no evidence that this does them any good.
Toward more precise care in hemodialysis
A first step toward more precise care might be to stop enforcing guidelines that are not based on solid evidence. Such an approach has recently been advocated by the International Society of Peritoneal Dialysis. Routine assessment of toxin removal is still recommended using urea or creatinine as surrogates but a peritoneal dialysis patient who is feeling well is not, however, obliged to increase the volume or frequency of exchanges to meet a numeric target.
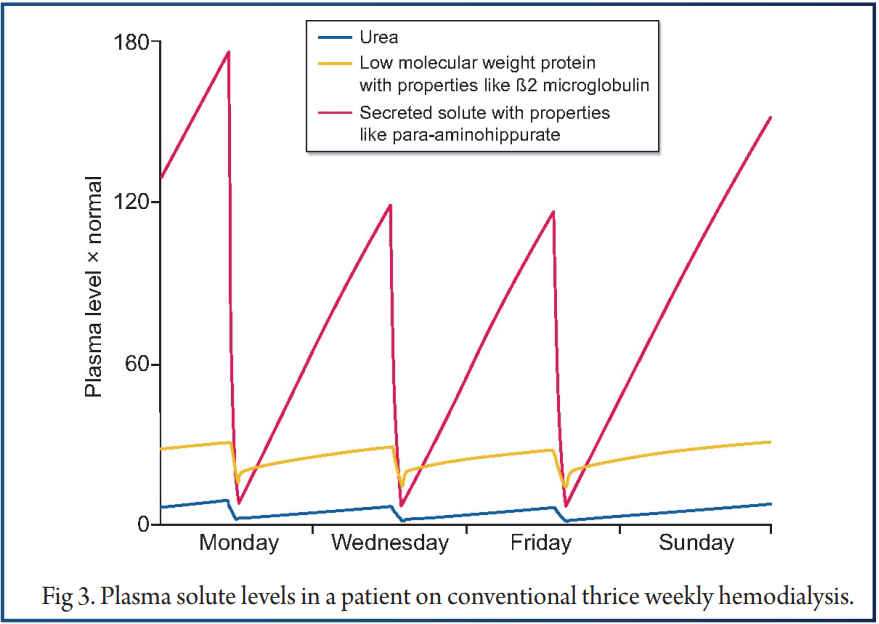
However, patients who feel well and have adequate volume and inorganic ion control would not be obliged to spend more time on hemodialysis to achieve a urea kinetic target. It has the highest dialytic clearance of any known solute but in contrast the native kidney clears many solutes more rapidly than urea, which is in part reabsorbed in the proximal tubule. As a result, levels of other solutes remain much higher relative to normal than urea levels in patients maintained on standard hemodialysis, as depicted in Figure 3.
However, the assessment of hemodialysis adequacy by urea removal has inhibited study of potential toxins that are less effectively cleared by hemodialysis, and discouraged development of new means to remove them. Simultaneous determination of large numbers of solutes will be required to identify toxins responsible for various features of uremic illness.
Quantification of clinical endpoints associated with solute levels presents a more difficult problem. Several strategies can be envisioned. The first, which is now being pursued, is to analyze samples from large numbers of patients and rely on statistical methods to distinguish illness due to uremic solutes from the comorbid processes prevalent in the hemodialysis population. Large studies would be required to distinguish the value of reducing solute levels in patients with different comorbidities.
Conclusions
In conclusion, we have discussed how therapeutic choices are progressing toward completely customised approaches for patients with end-stage renal failure. Kidney transplantation is without a doubt the most effective form of renal replacement treatment, and significant progress has been made in molecular risk prediction and subsequent personalised immunosuppressive pharmacodynamics. Given the broad alloimmune response to hla and non-hla epitopes, we are certain that only tolerance induction, such as through mixed chimerism, has the potential to significantly improve graft survival.
Hemodialysis, on the other hand, hasn’t seen many sophisticated treatments in recent years, and there’s still a lot of study to be done on the toxicity of uremic solutes produced from the gastrointestinal system.
References
1. Patel R, Terasaki PI. Signiffcance of the positive crossmatch test in kidney transplantation. N Engl J Med 1969; 280: 735–739
2. Solez K, Racusen LC, Marcussen N et al. Morphology of ischemic acute renal failure, normal function, and cyclosporine toxicity in cyclosporine-treated renal allograft recipients. Kidney Int 1993; 43: 1058–1067
3. Mengel M, Sis B, Haas M, et al. ; Bantt meeting report writing committee. Banff 2011 Meeting report: new concepts in antibody-mediated rejection. Am J Transplant 2012; 12: 563–570
4. Wekerle T, Segev D, Lechler R et al. Strategies for long-term preservation of kidney graft function. Lancet 2017; 389: 2152–2162
5. Wiebe C, Rush DN, Nevins TE et al. Class II eplet mismatch modulates tacrolimus trough levels required to prevent donor-specific antibody development. J Am Soc Nephrol 2017; 28: 3353–3362
6. Engen RM, Jedraszko AM, Conciatori MA et al. Substituting imputation of HLA antigens for high resolution HLA typing: evaluation of a multiethnic population and implications for clinical decision making in transplantation. Am J Transplant 2020 (published online 20 May); doi: 10.1111/ajt.16070
7. de Klerk M, Kal-van Gestel JA, van de Wetering J et al. Creating options for difficult-to-match kidney transplant candidates. Transplantation 2020 (published online February); doi: 10.1097/tp.0000000000003203
8. Rees MA, Dunn TB, Kuhr CS et al. Kidney exchange to overcome financial barriers to kidney transplantation. Am J Transplant 2017; 17: 782–790
9. Opelz G; Collaborative Transplant Study. Non-HLA transplantation immunity revealed by lymphocytotoxic antibodies. Lancet 2005; 365: 1570–1576
10. Reindl-Schwaighofer R, Heinzel A, Kainz A et al. Contribution of non-HLA incompatibility between donor and recipient to kidney allograft survival: genome-wide analysis in a prospective cohort. Lancet 2019; 393: 910–91711.
11. Steers NJ, Li Y, Drace Z et al. Genomic mismatch at LIMS1 locus and kidney allograft rejection. N Engl J Med 2019; 380: 1918–1928
12. Mahr B, Granofszky N, Muckenhuber M et al. Transplantation tolerance through hematopoietic chimerism: progress and challenges for clinical translation. Front Immunol 2017; 8: 1–14
13. LoCascio SA, Morokata T, Chilfenden M et al. Mixed chimerism, lymphocyte recovery, and evidence for early donor-specific unresponsiveness in patients receiving combined kidney and bone marrow transplantation to induce tolerance. Transplantation 2010; 90: 1607–1615
14. Chaudhry S, Kato Y, Weiner J et al. Transient mixed chimerism with nonmyeloablative conditioning does not induce liver allograft tolerance in nonhuman primates. Transplantation 2020 (published online 6 April); doi: 10.1097/TP.0000000000003263


