
Introduction
Therapeutic treatments for desensitisation and antibody-mediated rejection (AMR) in patients with preformed or de novo donor-specific HLA antibodies are urgently needed (DSA). Due to preformed DSA identified at the time of transplant or the reactivation of HLA memory after transplantation, the risk of AMR and allograft loss in sensitised individuals is enhanced, resulting in acute and chronic AMR.
De novo DSA, which develops after a transplant owing to insufficient immunosuppression, can result in acute and chronic AMR, as well as allograft loss. Desensitization and AMR treatment have mostly targeted circulating antibody, the ultimate result of the humoral immune response.
However, in many cases, these treatments fail to effectively remove all DSA, and patients with residual DSA have significantly worse long-term results than non-sensitized individuals. Targeting several components of humoral immunity, we believe, will enhance outcomes for these individuals. We will briefly cover traditional desensitisation techniques that target antibody or B cell elimination in this review, before presenting a mechanistically designed desensitisation regimen that targets plasma cells and the humoral response.
The Current Desensitization Treatment Strategy
Plasmapheresis or Immunoadsorption
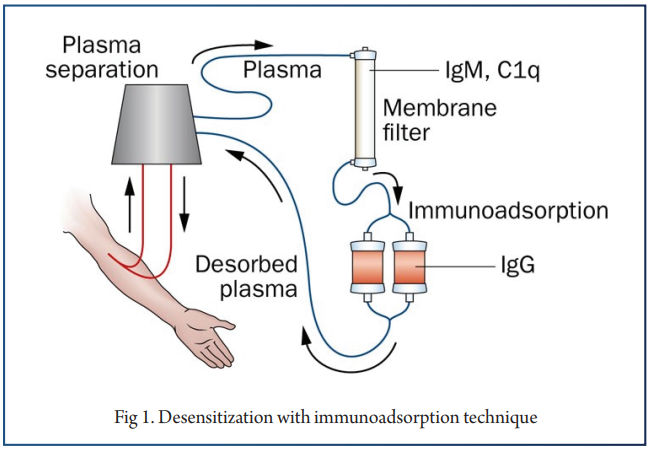
Plasmapheresis (PP) has been used for several decades as a method for lowering circulating antibody in various immune diseases. Using the double filtration plasmapheresis (DFPP) system, a cascade of filtration traps larger molecules, and thus allow lower molecular weight components to pass back to the patient.
Together with IVIg, it has been used to effect successful transplantation for positive crossmatch patients, and for many units, is the mainstay of desensitization prior to transplantation. The kinetics of antibody removal by PP are predictable within limited periods compared with other treatment modalities since plasma proteins are reliably removed. Therefore, PP or IA can be used as an effective treatment modality in the setting of planned transplantation across a positive HLA cross-match in living donor KT (Fig 1).
Intravenous Immunoglobulin
IVIG has been widely used in inflammatory and autoimmune conditions. Although widely used as part of desensitization regimens for many decades, the precise mechanism of action is unknown as a result of its broad spectrum of effects.
Many potential mechanisms of action of IVIG in transplantation have been proposed. IVIG has been used in various doses according to protocol from 100mg/kg to 2.0g/kg in desensitization prior to living donor KT or for deceased donor KT of patients with high PRA. Although various combinations of IVIG or PP with rituximab have been proposed, two protocols have been widely accepted and used.
PP With Low-Dose IVIG vs. High-Dose IVIG Alone
Using PP with low-dose IVIG, many centers report transplant outcomes with acute AMR rates of 12-43% when used in combination with various induction agents, anti-thymocyte globulin, anti-IL-2Rc antibody or OTK3. The NIH IGO2 study, a controlled clinical, multi-center, double blinded trial of IVIG (2g/kg, monthly 4 times) versus placebo in sensitized patients, HLA antibody levels were reduced further, and the transplantation rate was higher in the IVIG group than in the placebo group.
Reported successful transplantation outcomes with two doses of 2mg/kg IVIG on day 0 and day 30 with rituximab in 20 patients. Among 76 patients with PRA ≥30%, 31 patients received living donor KT, and 45 patients received deceased donor KT with reduced waiting time of 4.2 ± 4.5 months.
Anti-CD20 Antibody (Rituximab)
Rituximab is an anti-CD20 monoclonal antibody that binds to CD20 expressed on immature and mature B-lymphocytes, inducing apoptosis via antibody-dependent cytotoxicity, complement-dependent cytotoxicity or direct apoptosis.
Originally, anti-CD 20 antibody was used to treat B-cell lymphoma. Rituximab has been used as an additional therapy as part of desensitization treatments, in conjunction with plasmapheresis & IvIg. The half-life of rituximab in patients with end-stage renal disease is known to be 9-14 days.
New Pharmacologic Strategies for Desensitization
Targeting Antibodies
IgG Endopeptidases
More recently, attempts have been made to fundamentally alter the structure of preformed antibody, using IgG endopeptidase (IdeS) which is a bacterial enzyme produced by S. pyogenes that cleaves all four human IgG subclasses into F(ab) & F (c) fragments, thus inhibiting both complement-dependent cytotoxicity and antibody-dependent cytotoxicity (Fig 2).
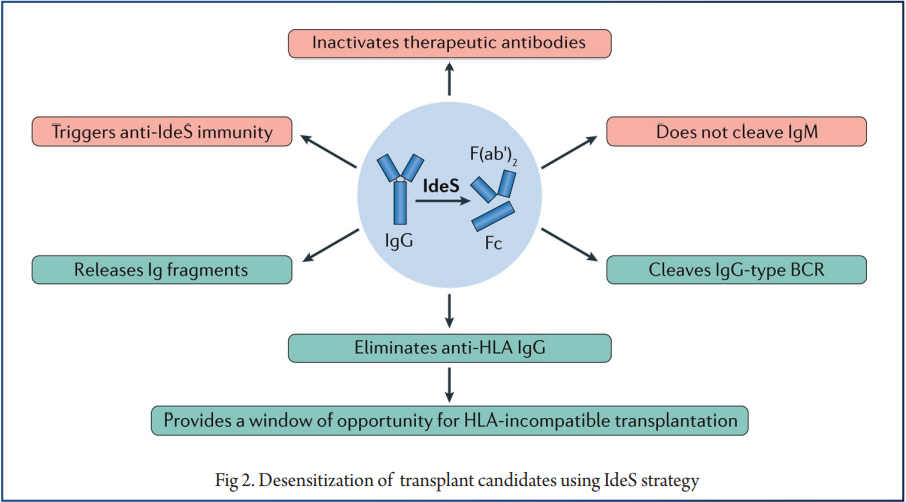
Recently completed a trial of IdeS in 25 highly sensitized patients prior to HLA-incompatible kidney transplantation. All patients had near-complete or complete reductions of anti-HLA antibodies and donor-specific antibodies at 24 hours post-transplant, which allowed successful transplantation in 24/25 (96%). These findings suggest that IdeS has strong, albeit transient, ability to reduce DSA that may make this therapy useful in combination with strategies that allow for longer-term control of DSA rebound.
Anti-FcRn Approach
Identified FcRn, a neonatal IgG receptor that is closely related to the MHC Class I receptor, which is involved in a variety of critical biological and immunological functions, most notably regulating serum IgG levels and the recycling and transcytosis process that results in an increased half-life of IgG and albumin in human serum.
IVIG was one of the first therapies to decrease anti-HLA antibodies and treat antibody-mediated autoimmune diseases through blocking the IgG-FcRn pathway, leading to saturation of FcRn receptors and degradation of IgG molecules. Since then, multiple therapies targeting FcRn or the IgG-FcRn interaction have been developed as treatment for autoimmune and infectious diseases, with promising benefits as therapeutic agents in reducing AMR in transplantation.
Rozanolixizumab is a high affinity anti-human neonatal FcRn mAb that reduced plasma IgG concentrations in cynomologus monkeys by up to 85%. Phase II clinical trials of Rozanolixizumab were recently completed in patients with immune thrombocytopenia and myasthenia gravis.
Targeting Plasma Cells
Targeting Plasma cells with Proteasome Inhibition
Bortezomib is a 1st generation, reversible inhibitor of the 26S proteasomal subunit. This drug is a potent inhibitor of plasma cells, which rely on rapid protein turnover to continually secrete antibodies, and succumb to oxidative stress and apoptosis when cellular recycling mechanisms are rendered nonfunctional. For this reason, bortezomib is approved for usage in multiple myeloma, a malignancy of plasma cells.
Studies described its use as effective treatment of AMR and ACR as well as reduction in DSA in kidney transplant recipients. and Mulder et al. Following some success for usage in refractory antibody-mediated rejection after kidney transplantation, several groups have used bortezomib in the context of desensitization.
Used a combination of high dose IVIG, rituximab, and bortezomib and demonstrated a small reduction in the MFI value of class I PRA, and an increased rate of deceased donor kidney transplantation with no graft loss in the desensitized group at a median follow-up of 23 months.
Immunoproteasome Inhibitors
Conventional PIs are broad spectrum PIs with various dose-dependent adverse effects. An attractive alternative would be to solely target the proteasome of immune cells.
Therefore, inhibition of the immunoproteasome allows for both the targeting of immune-specific cells but also cells actively involved in the inflammatory response. Newly developed immunoproteasome inhibitors (IPI) could selectively inhibit proteasomes of cells involved in graft rejection after transplantation, such as B and T lymphocytes and APC’s, and regulate pro-inflammatory cytokines and the differentiation of helper T cells.
But similar to conventional PIs, PC population would be more sensitive on IPIs. ONX-0914, formerly known as PR-957, is an LMP7-selective immunoproteasome inhibitor that is undergoing clinical studies in the treatment of autoimmune diseases and has potential applications in transplantation.
Monoclonal Antibodies for Targeting Plasma Cells
Inhibiting proteasome activity with PI should affect more than plasma cell population since all eukaryotic cells utilize proteasome to maintain their homeostasis. Even IPI should have broad impact on immune cells.Therefore, monoclonal antibody targeting of plasma cell population is very attractive. There are only anecdotal cases evaluating monoclonal antibodies targeting PC in organ transplantation to prevent or treat antibody-mediated rejection.
In our sensitized NHP model, study reported the effectiveness of daratumumab in combination with an anti-CXCR4 antagonist, plerixafor which mobilizes PC from bone marrow to peripheral blood. Currently, there is a phase 1 clinical trial to evaluate daratumumab in decreasing circulating antibodies in sensitized recipients awaiting heart transplantation.
There is also a clinical trial to evaluate the safety and efficacy of isatuximab as desensitization therapy in patients awaiting kidney transplantation. If applied to transplant, these therapies from myeloma field need be carefully evaluated on their off-target effect in a transplantation setting.
Targeting Mediators/Survival Factor
Interleukin-6 Receptor Inhibition
IL-6 is critical for many inflammatory pathways and has a key role in the induction of follicular helper T cells, which direct naïve B cells in the germinal center to differentiate to memory B cells and high-affinity, IgG-secreting plasma cells. IL-6 has also been associated with deviation of T cells towards a Th17 phenotype, reduction of the proportion of Treg cells, and potentiation of allograft rejection in kidney transplantation.
Pharmacologic inhibition of IL-6 signaling is attractive in the context of desensitization strategies, as animal models have shown that this therapy reduces alloantibody responses by inhibition of bone marrow plasma cells and induction of Treg cells.
Anti-BAFF Agents
B cell activating factor (BAFF) is a homotrimer and member of the tumor necrosis factor (TNF) family that is found on the cell surface as a transmembrane protein or released in soluble form after cleavage. Therefore, blocking this molecule may be essential when targeting allo-B cell response. A monoclonal antibody against BAFF, belimumab, was the first targeted biologic approved for the treatment of systemic lupus erythematosus. Blisibimod is a second anti-Baff agent developed for SLE. While considerable progress has been made in the field of desensitization, many potential and untested therapies remain.
Multi-Modal Approach to Desensitization
The conventional desensitization concept, removal of preformed antibody, may prevent hyperacute rejection or acute AMR but without long-lasting impact on humoral alloimmunity. While many desensitization therapies have been tried alone or in combination in animal models and human trials, none yet have solved the barriers to transplantation faced by highly sensitized patients with high titer HLA antibodies.
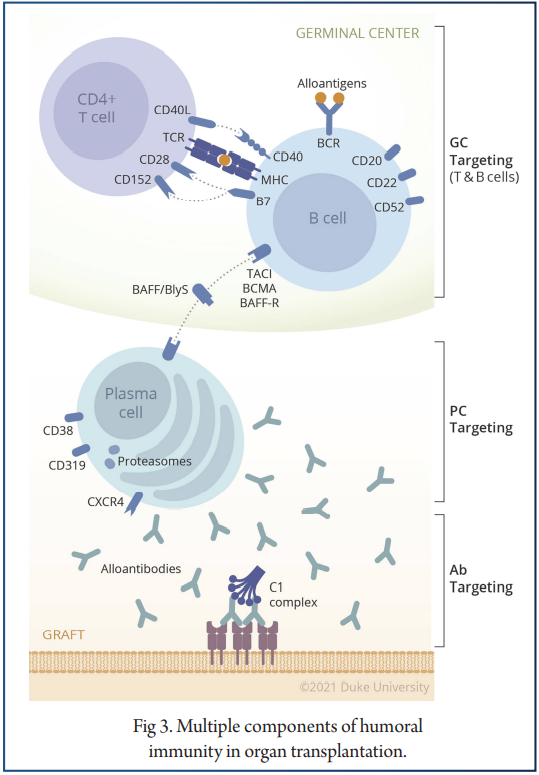
The answer to desensitization may lie in novel therapies not yet tested or those outside the field of transplantation. For this reason, targeting each component of humoral response such as alloantibody, B cells, or PC, would tentatively reduce the steady state level of DSA, this would not promote long-term control of humoral response after transplantation. Due to its compensatory mechanism, it would more logical that we develop strategies to desensitizing patients that target multiple steps of DSA production. Fortunately, there are many agents targeting each step of the humoral response as shown in Fig 3.
Conclusion
As there are too many potential combinations of biologics, it is necessary to permit exhaustive evaluation of each possible combination. Therefore, rational approaches merit testing in a preclinical model before being translated into the clinic.
References
- Patel R, Terasaki PI. Significance of the Positive Crossmatch Test in Kidney Transplantation. New Engl J Med (1969) 280:735–9. doi: 10.1056/NE- JM196904032801401
- Loupy A, Lefaucheur C. Antibody-Mediated Rejection of Solid-Organ Allografts. N Engl J Med (2018) 379:1150–60. doi: 10.1056/NEJMra1802677
- Valenzuela NM, Reed EF. Antibody-Mediated Rejection Across Solid Organ Transplants: Manifestations, Mechanisms, and Therapies. J Clin Invest (2017) 127:2492–504. doi: 10.1172/JCI90597
- Yabu JM, Anderson MW, Kim D, Bradbury BD, Lou CD, Petersen J, et al. Sensitization From Transfusion in Patients Awaiting Primary Kidney Transplant. Nephrology, Dialysis, Transplantation: Official Publication of the European Dialysis and Transplant Association – European Renal Association. Nephrol Dialysis Transpl (2013) 28:2908–18. doi: 10.1093/ndt/gft362
- Higgins R, Lowe D, Daga S, Hathaway M, Williams C, Lam FT, et al. Pregnancy-Induced HLA Antibodies Respond More Vigorously After Renal Transplantation Than Antibodies Induced by Prior Transplantation. Hum Immunol (2015) 76:546–52. doi: 10.1016/j.humimm.2015.06.013
- Picascia A, Grimaldi V, Sabia C, Napoli C. Comprehensive Assessment of Sensitizing Events and Anti-HLA Antibody Development in Women Awaiting Kidney Transplantation. Transpl Immunol (2016) 36:14–9. doi: 10.1016/j.trim.2016.03.002
- El-Awar N, Terasaki P, Lazda V, Nikaein A, Manning C, Arnold AN. Almost All Patients Who Are Waiting for a Regraft of a Kidney Transplant Have Anti-HLA Antibodies. Transplant Proc (2002) 34:2531–2. doi: 10.1016/S0041-1345(02)03520-0
- Cecka JM, Calculated PRA. (CPRA): The New Measure of Sensitization for Transplant Candidates. Am J Transplant Off J Am Soc Transplantationand Am Soc Transplant Surgeons (2010) 10:26–9. doi: 10.1111/j.1600-6143.2009.02927.
- Matas AJ, Smith JM, Skeans MA, Thompson B, Gustafson SK, Stewart DE, et al. Optn/Srtr 2013 Annual Data Report: Kidney. Am J Transplant (2015)
- Pruthi R, Hilton R, Pankhurst L, Mamode N, Hudson A, Roderick P, et al. Uk Renal Registry 16th Annual Report: Chapter 4 Demography of Patients Waitlisted for Renal Transplantation in the UK: National and Centre-Specific Analyses. Nephron Clin Pract (2013) 125:81–98. doi: 10.1159/000360023
- Claas FH, Witvliet MD, Duquesnoy RJ, Persijn GG, Doxiadis II. The Acceptable Mismatch Program as a Fast Tool for Highly Sensitized Patients Awaiting a Cadaveric Kidney Transplantation: Short Waiting Time and Excellent Graft Outcome. Transplantation (2004) 78:190–3. doi: 10.1097/01.TP.0000129260.86766.67
- Bray RA, Gebel HM. The New Kidney Allocation System (KAS) and the Highly Sensitized Patient: Expect the Unexpected. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surgeons (2014) 14:2917. doi: 10.1111/ajt.12974
- Parsons RF, Locke JE, Redfield RR 3rd, Roll GR, Levine MH. Kidney Transplantation of Highly Sensitized Recipients Under the New Kidney Allocation System: A Reflection From Five Different Transplant Centers Across the United States. Hum Immunol (2017) 78:30–6. doi: 10.1016/j.humimm.2016.10.009
- Gebel HM, Kasiske BL, Gustafson SK, Pyke J, Shteyn E, Israni AK, et al. Allocating Deceased Donor Kidneys to Candidates With High Panel-Reactive Antibodies. Clin J Am Soc Nephrol (2016) 11:505–11. doi: 10.2215/CJN.07720715
- Gentry SE, Segev DL, Montgomery RA. A Comparison of Populations Served by Kidney Paired Donation and List Paired Donation. Am J Transplant (2005) 5:1914–21. doi: 10.1111/j.1600-6143.2005.00964.
- Ferrari P, Fidler S, Holdsworth R, Woodroffe C, Tassone G, Watson N, et al. High Transplant Rates of Highly Sensitized Recipients With Virtual Crossmatching in Kidney Paired Donation. Transplantation (2012) 94:744–9. doi: 10.1097/TP.0b013e3182612967
- Montgomery RA, Lonze BE, Jackson AM. Using Donor Exchange Paradigms With Desensitization to Enhance Transplant Rates Among Highly Sensitized Patients. Curr Opin Organ Transplant (2011) 16:439–43. doi: 10.1097/MOT.0b013e32834897c1
- Orandi BJ, Luo X, Massie AB, Garonzik-Wang JM, Lonze BE, Ahmed R, et al. Survival Benefit With Kidney Transplants From HLA-Incompatible Live Donors. New Engl J Med (2016) 374:940–50. doi: 10.1056/nejmoa1508380
- Manook M, Koeser L, Ahmed Z, Robb M, Johnson R, Shaw O, et al. Post-Listing Survival for Highly Sensitised Patients on the UK Kidney Transplant Waiting List: A Matched Cohort Analysis. Lancet (2017) 389(10070):727–34. doi: 10.1016/S0140-6736(16)31595-1
- Yazdi MF, Baghianimoghadam M, Nazmiyeh H, Ahmadabadi AD, Adabi MA. Response to Plasmapheresis in Myasthenia Gravis Patients: 22 Cases Report. Rom J Intern Med (2012) 50:245–7.
- Pusey CD, Levy JB. Plasmapheresis in Immunologic Renal Disease. Blood Purif (2012) 33:190–8. doi: 10.1159/000334155
- Higgins R, Lowe D, Hathaway M, Lam FT, Kashi H, Tan LC, et al. Double Filtration Plasmapheresis in Antibody-Incompatible Kidney TransplantationTherapeutic Apheresis and Dialysis : Official Peer-Reviewed Journal of the International Society for Apheresis, the Japanese Society for Apheresis, the Japanese Society for Dialysis Therapy. Ther Apher Dialysis (2010) 14:392–9. doi: 10.1111/j.1744-9987.2010.00821.
- Montgomery RA, Zachary AA, Racusen LC, Leffell MS, King KE, Burdick J, et al. Plasmapheresis and Intravenous Immune Globulin Provides Effective Rescue Therapy for Refractory Humoral Rejection and Allows Kidneys to be Successfully Transplanted Into Cross-Match-Positive Recipients. Transplantation (2000) 70:887–95. doi: 10.1097/00007890-200009270-00006


