
Introduction
The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes” includes the ADA’s current clinical practice recommendations and is intended to provide the components of diabetes care, general treatment goals and guidelines, and tools to evaluate quality of care.
Chronic Kidney Disease
Screening – Recommendations
11.1a – At least annually, urinary albumin (e.g., spot urinary albumin-to-creatinine ratio) and estimated glomerular filtration rate should be assessed in patients with type 1 diabetes with duration of ≥5 years and in all patients with type 2 diabetes regardless of treatment.
11.1b – Patients with diabetes and urinary albumin ≥300 mg/g creatinine and/or an estimated glomerular filtration rate 30–60 mL/min/1.73 m2 should be monitored twice annually to guide therapy.
Treatment – Recommendations
11.2 – Optimize glucose control to reduce the risk or slow the progression of chronic kidney disease.
11.3a – For patients with type 2 diabetes and diabetic kidney disease, use of a sodium–glucose cotransporter 2 inhibitor in patients with an estimated glomerular filtration rate ≥25 mL/min/1.73 m2 and urinary albumin ≥300 mg/g creatinine is recommended to reduce chronic kidney disease progression and cardiovascular events.
11.3b – In patients with type 2 diabetes and chronic kidney disease, consider use of sodium–glucose cotransporter 2 inhibitors additionally for cardiovascular risk reduction when estimated glomerular filtration rate and urinary albumin creatinine are ≥25 mL/min/1.73 m2 or ≥300 mg/g, respectively.
11.3c – In patients with chronic kidney disease who are at increased risk for cardiovascular events or chronic kidney disease progression or are unable to use a sodium–glucose cotransporter 2 inhibitor, a nonsteroidal mineralocorticoid receptor antagonist (finerenone) is recommended to reduce chronic kidney disease progression and cardiovascular events.
11.3d – In patients with chronic kidney disease who have ≥300 mg/g urinary albumin, a reduction of 30% or greater in mg/g urinary albumin is recommended to slow chronic kidney disease progression.
11.4 – Optimization of blood pressure control and reduction in blood pressure variability to reduce the risk or slow the progression of chronic kidney disease is recommended.
11.5 – Do not discontinue renin-angiotensin system blockade for minor increases in serum creatinine (≤30%) in the absence of volume depletion.
11.6 – For people with nondialysis-dependent stage 3 or higher chronic kidney disease, dietary protein intake should be a maximum of 0.8 g/kg body weight per day (the recommended daily allowance). A For patients on dialysis, higher levels of dietary protein intake should be considered, since malnutrition is a major problem in some dialysis patients.
11.7 – In nonpregnant patients with diabetes and hypertension, either an ACE inhibitor or an angiotensin receptor blocker is recommended for those with modestly elevated urinary albumin-to-creatinine ratio (30–299 mg/g creatinine) B and is strongly recommended for those with urinary albumin-to-creatinine ratio ≥300 mg/g creatinine and/or estimated glomerular filtration rate <60 mL/min/1.73 m2.
11.8 – Periodically monitor serum creatinine and potassium levels for the development of increased creatinine or changes in potassium when ACE inhibitors, angiotensin receptor blockers, or diuretics are used.
11.9 – An ACE inhibitor or an angiotensin receptor blocker is not recommended for the primary prevention of chronic kidney disease in patients with diabetes who have normal blood pressure, normal urinary albumin-to-creatinine ratio (<30 mg/g creatinine), and normal estimated glomerular filtration rate.
11.10 – Patients should be referred for evaluation by a nephrologist if they have an estimated glomerular filtration rate <30 mL/min/1.73 m2.
11.11 – Promptly refer to a nephrologist for uncertainty about the etiology of kidney disease, difficult management issues, and rapidly progressing kidney disease.
Epidemiology of Diabetes and Chronic Kidney Disease
Chronic kidney disease (CKD) is diagnosed by the persistent elevation of urinary albumin excretion (albuminuria), low estimated glomerular filtration rate (eGFR), or other manifestations of kidney damage. Diabetic kidney disease typically develops after diabetes duration of 10 years in type 1 diabetes but may be present at diagnosis of type 2 diabetes.
Assessment of Albuminuria and Estimated Glomerular Filtration Rate
Screening for albuminuria can be most easily performed by urinary albumin-to-creatinine ratio (UACR) in a random spot urine collection. Hence, it is better to simply collect a spot urine sample for albumin-to-creatinine ratio because it will ultimately need to be done. However, UACR is a continuous measurement, and differences within the normal and abnormal ranges are associated with renal and cardiovascular outcomes.
Furthermore, because of high biological variability of >20% between measurements in urinary albumin excretion, two of three specimens of UACR collected within a 3- to 6-month period should be abnormal before considering a patient to have high or very high albuminuria. Exercise within 24 h, infection, fever, congestive heart failure, marked hyperglycemia, menstruation, and marked hypertension may elevate UACR independently of kidney damage. eGFR should be calculated from serum creatinine using a validated formula.
Diagnosis of Diabetic Kidney Disease
Diabetic kidney disease is usually a clinical diagnosis made based on the presence of albuminuria and/or reduced eGFR in the absence of signs or symptoms of other primary causes of kidney damage. The typical presentation of diabetic kidney disease is considered to include a long-standing duration of diabetes, retinopathy, albuminuria without gross hematuria, and gradually progressive loss of eGFR.
An active urinary sediment (containing red or white blood cells or cellular casts), rapidly increasing albuminuria or nephrotic syndrome, rapidly decreasing eGFR, or the absence of retinopathy (in type 1 diabetes) suggests alternative or additional causes of kidney disease. For patients with these features, referral to a nephrologist for further diagnosis, including the possibility of kidney biopsy, should be considered. It is rare for patients with type 1 diabetes to develop kidney disease without retinopathy.
Staging of Chronic Kidney Disease
Stages 1–2 CKD have been defined by evidence of high albuminuria with eGFR ≥60 mL/min/1.73 m2, while stages 3–5 CKD have been defined by progressively lower ranges of eGFR (Fig. 11.1).

Acute Kidney Injury
People with diabetes are at higher risk of AKI than those without diabetes. Other risk factors for AKI include preexisting CKD, the use of medications that cause kidney injury (e.g., nonsteroidal anti-inflammatory drugs), and the use of medications that alter renal blood flow and intrarenal hemodynamics. There was concern that sodium–glucose cotransporter 2 (SGLT2) inhibitors may promote AKI through volume depletion, particularly when combined with diuretics or other medications that reduce glomerular filtration .
However, this has not been found to be true in randomized clinical outcome trials of advanced kidney disease or high cardiovascular disease risk with normal kidney function. Timely identification and treatment of AKI is important because AKI is associated with increased risks of progressive CKD and other poor health outcomes. Small elevations in serum creatinine (up to 30% from baseline) with renin-angiotensin system (RAS) blockers (such as ACE inhibitors and ARBs) must not be confused with AKI.
Accordingly, ACE inhibitors and ARBs should not be discontinued for minor increases in serum creatinine (<30%), in the absence of volume depletion. Lastly, it should be noted that ACE inhibitors and ARBs are commonly not dosed at maximally tolerated doses because of fear that serum creatinine will rise. Note that in all clinical trials demonstrating efficacy of ACE inhibitors and ARBs in slowing kidney disease progression, the maximally tolerated doses were used not very low doses that do not provide benefit.
Surveillance
Both albuminuria and eGFR should be monitored annually to enable timely diagnosis of CKD, monitor progression of CKD, detect superimposed kidney diseases including AKI, assess risk of CKD complications, dose drugs appropriately, and determine whether nephrology referral is needed. Among people with existing kidney disease, albuminuria and eGFR may change due to progression of CKD, development of a separate superimposed cause of kidney disease, AKI, or other effects of medications, as noted above.
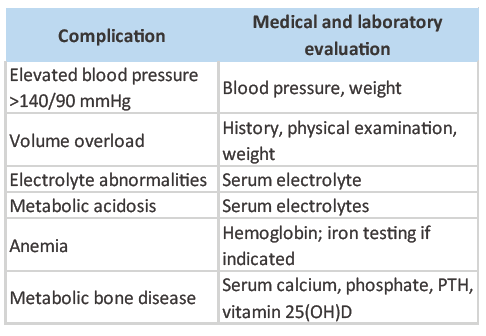
Serum potassium should also be monitored in patients treated with diuretics because these medications can cause hypokalemia, which is associated with cardiovascular risk and mortality. For patients with eGFR <60 mL/min/1.73 m2, those receiving ACE inhibitors, ARBs, or MRAs should have serum potassium measured periodically. Additionally, people with this lower range of eGFR should have appropriate medication dosing verified, exposure to nephrotoxins (e.g., nonsteroidal anti-inflammatory drugs and iodinated contrast) should be minimized, and potential CKD complications should be evaluated (Table 1).
Referral to a Nephrologist
Consider referral to a nephrologist when there is uncertainty about the etiology of kidney disease, for difficult management issues (anemia, secondary hyperparathyroidism, significant increases in albuminuria in spite of good blood pressure control, metabolic bone disease, resistant hypertension, or electrolyte disturbances), or when there is advanced kidney disease (eGFR <30 mL/min/1.73 m2) requiring discussion of renal replacement therapy for ESRD .
The threshold for referral may vary depending on the frequency with which a provider encounters patients with diabetes and kidney disease. Consultation with a nephrologist when stage 4 CKD develops (eGFR <30 mL/min/1.73 m2) has been found to reduce cost, improve quality of care, and delay dialysis. However, other specialists and providers should also educate their patients about the progressive nature of CKD, the kidney preservation benefits of proactive treatment of blood pressure and blood glucose, and the potential need for renal replacement therapy.
References:
1. Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA Consensus Conference. Diabetes Care 2014;37:2864–2883.
2. National Kidney Foundation. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013;3:1–150.
3. Afkarian M, Zelnick LR, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA 2016;316:602–610.
4. de Boer IH, Rue TC, Hall YN, Heagerty PJ, Weiss NS, Himmelfarb J. Temporal trends in the prevalence of diabetic kidney disease in the United States. JAMA 2011;305:2532–2539.
5. de Boer IH; DCCT/EDIC Research Group. Kidney disease and related findings in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study. Diabetes Care 2014;37:24–30.
6. Johansen KL, Chertow GM, Foley RN, et al. US Renal Data System 2020 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis 2021;77(Suppl. 1):A7–A8.
7. Fox CS, Matsushita K, Woodward M, et al.; Chronic Kidney Disease Prognosis Consortium. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: a metaanalysis. Lancet 2012;380:1662–1673.
8. Yarnoff BO, Hoerger TJ, Simpson SK, et al.; Centers for Disease Control and Prevention CKD Initiative. The cost-effectiveness of using chronic kidney disease risk scores to screen for early-stage chronic kidney disease. BMC Nephrol 2017;18:85.
9. Coresh J, Heerspink HJL, Sang Y, et al.; Chronic Kidney Disease Prognosis Consortium and Chronic Kidney Disease Epidemiology Collaboration. Change in albuminuria and subsequent risk of endstage kidney disease: an individual participant-level consortium meta analysis of observational studies. Lancet Diabetes Endocrinol 2019;7:115–127.
10. Levey AS, Gansevoort RT, Coresh J, et al. Change in albuminuria and GFR as end points for clinical trials in early stages of CKD: a scientific workshop sponsored by the National Kidney Foundation in collaboration with the US Food and Drug Administration and European Medicines Agency. Am J Kidney Dis 2020;75:84–104.
11. Afkarian M, Sachs MC, Kestenbaum B, et al. Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol 2013;24:302–308.
12. Groop P-H, Thomas MC, Moran JL, et al.; FinnDiane Study Group. The presence and severity of chronic kidney disease predicts allcause mortality in type 1 diabetes. Diabetes 2009;58:1651–1658.


