
Abstract
Recent advances in surgical, immunosuppressive and monitoring protocols have led to the significant improvement of overall one-year kidney allograft outcomes. Chronic and acute antibody mediated rejection and non-immunological complications following kidney transplantation, including multiple incidences of primary kidney disease, as well as complications such as cardiovascular diseases, infections, and malignancy are the major factors that have contributed to the failure of kidney allografts. The use of molecular techniques to enhance histological diagnostics and noninvasive surveillance are what the latest studies in the field of clinical kidney transplant seem to mainly focus upon. Increasingly innovative approaches are being used to discover immunosuppressive methods to overcome critical sensitization, prevent the development of anti-human leukocyte antigen antibodies, treat chronic active ABMR, and reduce non-immunological complifications following kidney transplantation. In this article, we discuss the recent research developments in kidney transplantation that may impact long-term allografts and patient survival, as well as the latest developments in living kidney donation.
Non-HLA Antibodies in Transplantation
Human leukocyte antigens (HLA) are considered the most important non-self allo-antigens in organ transplantation. In addition, patients can form antibodies against targets other than HLA .
Multiple targets for these non-HLA antibodies have been studied in kidney transplantation over the last decade (Figure 1).

Active AMR
Chronic active ABMR is one of the major causes of long-term allograft loss. Tocilizumab, a humanized monoclonal antibody targeting the interleukin-6 receptor, has been assessed in patients with acute and chronic active ABMR given that IL-6 mediates various inflammatory and immunomodulatory pathways, including the expansion and activation of T cells and B cells. There is a genetically engineered humanized ImmunoglobulinG1 monoclonal antibody that binds to IL-6, inhibiting its interaction with IL-6R. Direct inactivation of IL-6 may limit a rebound induced by the accumulafition of IL-6. Preliminary investigations from phase 1-2 trials demonstrated the effcacy of the C1q inhibitor for the prevention of a delayed graft function and to lessen athe occurrence of chronic active ABMR.
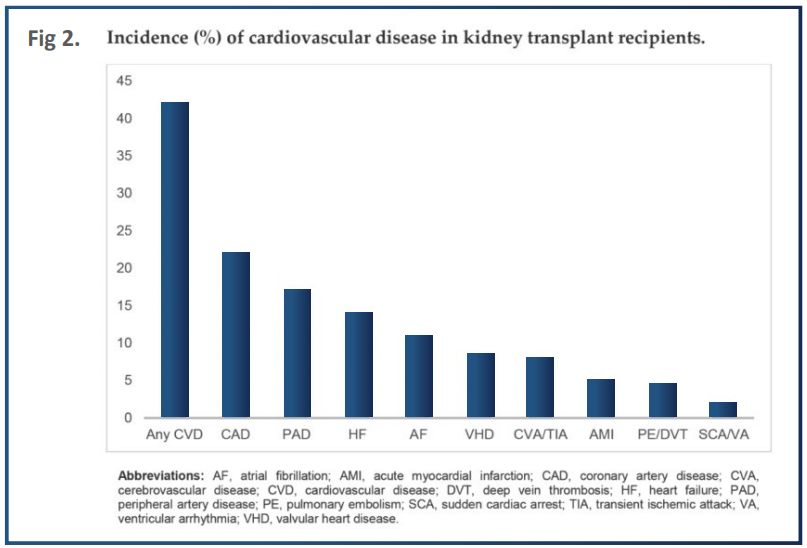
Cardiovascular Diseases in Kidney Transplant Recipients
The burden of cardiovascular diseases on ESKD is improved after kidney transplantation. However, it remains the leading cause of reduced early renal graft loss and mortality, as it is associated with significant morbidity and healthcare costs. Major phenotypes of cardiovascular diseases among kidney transplant recipients include ischemic heart disease, congestive heart failure, valvular heart disease, arrhythmias and pulmonary hypertension (Fig 2).
Preexisting Diabetes and Post Transplantation Diabetes
Preexisting diabetes and post-transplantation diabetes confer reduced patient and graft survival in kidney transplant recipients Hyperglycemia is present in nearly 90% of kidney transplant recipients in the immediate postoperative period, but it is not sustained in the majority. Some transplant immunosuppressive medications, including corticosteroids, calcineurin Inhibitors, and mammalian target of rapamycin inhibitors, are associated with a higher incidence of metabolic complications such as post-transplantation diabetes. Several studies have suggested the safe use of sodium glucose transport 2 inhibitors in kidney transplant recipients but future studies are needed as kidney transplant recipients are particularly susceptible to infections.
Post Transplant Malignancy
Cancer is one of the three major causes of death after kidney transplantation. The effect of viral infections, induction and immunosuppressive maintenance regimens have been proposed as important risk factors for post transplant malignancy. The increased risk of cancer may be due to viral reactivation induced by immunosuppressive agents. A higher degree of immunosuppression is associated with an increased risk of malignancy, and calcineurin inhibitors can promote carcinogenesis.
Infection
Solid organ transplant recipients are at greater risk of infection than the non-immunosuppressed population. Infections are the most common non-cardiovascular causes of mortality following kidney transplantation, accounting for 15%–20% of mortality. The first six months post-transplant is the time of greatest infection risk. Among all infectious complications, viruses are considered to be the most common agents. Herpes simplex virus, varicella zoster virus, BK polyomavirus, cytomegalovirus, Epstein–Barr virus, hepatitis B virus, and adenovirus are well-known etiologic agents of viral infections in kidney transplant patients worldwide. In order to prevent opportunistic infections in kidney transplant recipients, antimicrobial prophylaxis is recommended after kidney transplantation.
Latest Developments in Living Kidney Donation
Living donor kidney transplants are the best option for many patients with ESKD. Paired kidney donation provides living kidney donation for donor/recipient pairs that otherwise would not be feasible or need desensitization. Other possible approaches for increasing the donor pool include ABO-incompatible transplantation, the utilization of higher risk donors,
advanced donation with a voucher system, and providing donors with financial incentives. Living donors seem to have a higher risk of ESKD, particularly in obese donors and also for African American donors with an apolipoprotein L1 (APOL1) high-risk genotype. In African American living kidney donors, those with the APOL1 high-risk genotype had an almost three times more accelerated decline in estimated glomerular filtration rate (eGFR) after adjusting for pre-donation eGFR than those with a low-risk genotype.
Potential Directions and Future Scope
The most recent endeavors in kidney transplantation tend to mainly focus on noninvasive monitoring, as well as the improvement of histological diagnostics with the aid of molecular techniques. Such studies other creative means that can be used to find immunosuppressive agents, which can effectively overcome critical sensitization, prevent the creation of anti-HLA antibodies, treat chronic active ABMR, and reduce non-immunological complications following kidney transplantation, such as the recurrence of primary kidney disease and other complications. It is strongly believed that big data and artificial intelligence will reshape the research done on kidney transplantation in the near future. In addition, the utilization of telemedicine is increasing, providing benefits such as reaching out to kidney transplant patients in remote areas and helping to make scarce healthcare resources more accessible for kidney transplantation.
References
1. Abecassis M., Bartle S.T., Collins A.J., Davis C.L., Delmonico F.L., Friedewald J., Hays R., Howard A., Jones E., Leichtman A.B., et al. Kidney transplantation as primary therapy for end-stage renal disease: A National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQITM) conference. Clin. J. Am. Soc. Nephrol. 2008;3:471–480. doi: 10.2215/CJN.05021107.
2. Loupy A., Lefaucheur C., Vernerey D., Prugger C., Duong van Huyen J.P., Mooney N., Suberbielle C., Frémeaux-Bacchi V., Méjean A., Desgrandchamps F., et al. Complement-binding anti-HLA antibodies and kidney-allograft survival. N. Engl. J. Med. 2013;369:1215–1226. doi: 10.1056/NEJMoa1302506.
3. Viklicky O., Novotny M., Hruba P. Future developments in kidney transplantation. Curr. Opin. Organ Transplant. 2020;25:92–98. doi: 10.1097/- MOT.0000000000000722.
4. Faenza A., Fuga G., Nardo B., Donati G., Cianciolo G., Scolari M., Stefoni S. Metabolic Syndrome After Kidney Transplantation. Transplant. Proc. 2007;39:1843–1846. doi: 10.1016/j.transproceed.2007.07.019.
5. Cohen-Bucay A., Gordon C.E., Francis J.M. Non-immunological complications following kidney transplantation. F1000Research. 2019;8:194. doi: 10.12688/f1000research.16627.1.
6. Gill J.S., Abichandani R., Kausz A.T., Pereira B.J. Mortality after kidney transplant failure: The impact of non-immunologic factors. Kidney Int. 2002;62:1875–1883. doi: 10.1046/j.1523-1755.2002.00640.x.
7. Roedder S., Sigdel T., Salomonis N., Hsieh S., Dai H., Bestard O., Metes D., Zeevi A., Gritsch A., Cheeseman J., et al. The kSORT Assay to Detect Renal Transplant Patients at High Risk for Acute Rejection: Results of the Multicenter AART Study. PLoS Med. 2014;11:e1001759. doi: 10.1371/journal.pmed.1001759.
8. Garg N., Samaniego M.D., Clark D., Djamali A. Defining the phenotype of antibody-mediated rejection in kidney transplantation: Advances in diagnosis of antibody injury. Transplant. Rev. 2017;31:257–267. doi: 10.1016/j.trre.2017.08.005.
9. Bloom R.D., Bromberg J.S., Poggio E.D., Bunnapradist S., Langone A.J., Sood P., Matas A.J., Mehta S., Mannon R.B., Sharfuddin A., et al. Cell-Free DNA and Active Rejection in Kidney Allografts. J. Am. Soc. Nephrol. 2017;28:2221–2232. doi: 10.1681/ASN.2016091034.
10. Huang E., Sethi S., Peng A., Najjar R., Mirocha J., Haas M., Vo A., Jordan S.C. Early clinical experience using donor-derived cell-free DNA to detect rejection in kidney transplant recipients. Arab. Archaeol. Epigr. 2019;19:1663–1670. doi: 10.1111/ajt.15289.
11. Gielis E.M., Ledeganck K.J., Dendooven A., Meysman P., Beirnaert C., Laukens K., De Schrijver J., Van Laecke S., Van Biesen W., Emonds M.-P., et al. The use of plasma donor-derived, cell-free DNA to monitor acute rejection after kidney transplantation. Nephrol. Dial. Transplant. 2019;35:714–721. doi: 10.1093/ndt/gfz091.
12. Oellerich M., Shipkova M., Asendorf T., Walson P.D., Schauerte V., Menenmeyer N., Kabakchiev M., Hasche G., Gröne H., Friede T., et al. Absolute quantification of donor-derived cell-free DNA as a marker of rejection and graft injury in kidney transplantation: Results from a prospective observational study. Arab. Archaeol. Epigr. 2019;19:3087–3099. doi: 10.1111/ajt.15416.
13. Jordan S.C., Bunnapradist S., Bromberg J.S., Langone A.J., Hiller D., Yee J., Sninsky J.J., Woodward R., Matas A.J. Donor-derived Cell-free DNA Identifies Antibody-mediated Rejection in Donor Specific Antibody Positive Kidney Transplant Recipients. Transplant. Direct. 2018;4:e379. doi: 10.1097/TXD.0000000000000821.
14. Sigdel T., Archila F.A., Constantin T., Demko Z., Liberto J.M., Damm I., Towghi P., Navarro S., Kirkizlar E., Demko Z., et al. Optimizing Detection of Kidney Transplant Injury by Assessment of Donor-Derived Cell-Free DNA via Massively Multiplex PCR. J. Clin. Med. 2018;8:19. doi: 10.3390/jcm8010019.
15. Reeve J., Böhmig G.A., Eskandary F., Einecke G., Gupta G., Madill-Thomsen K., Mackova M., Halloran P.F. INTERCOMEX MMDx-Kidney study group Generating automated kidney transplant biopsy reports combining molecular measurements with ensembles of machine learning classifiers. Arab. Archaeol. Epigr. 2019;19:2719–2731. doi: 10.1111/ajt.15351.
16. Jordan S.C., Lorant T., Choi J. IgG Endopeptidase in Highly Sensitized Patients Undergoing Transplantation. N. Engl. J. Med. 2017;377:1693–1694. doi: 10.1056/NEJMoa1612567.
17. Lorant T., Bengtsson M., Eich T., Eriksson B.-M., Winstedt L., Järnum S., Stenberg Y., Robertson A.-K., Mosén K., Björck L., et al. Safety, immunogenicity, pharmacokinetics, and effcacy of degradation of anti-HLA antibodies by IdeS (imlidase) in chronic kidney disease patients. Arab. Archaeol. Epigr. 2018;18:2752–2762. doi: 10.1111/ajt.14733.
18. Bray R.A., Gebel H.M., Townsend R., Roberts M.E., Polinsky M., Yang L., Meier-Kriesche H.-U., Larsen C.P. De novo donor-specific antibodies in belatacept-treated vs cyclosporine-treated kidney-transplant recipients: Post hoc analyses of the randomized phase III BENEFIT and BENEFIT-EXT studies. Arab. Archaeol. Epigr. 2018;18:1783–1789. doi: 10.1111/ajt.14721


