
Introduction
Peritoneal Dialysis (PD) has become more popular in the last decade. Many of these individuals are transplant recipients who may require dialysis due to Delayed Graft Function (DGF). The effects of DGF based on post-transplantation dialysis are not well understood. DGF is defined as the necessity for dialysis within the first 7 days of receiving a kidney transplant. DGF is linked to negative outcomes such as acute rejection and poorer graft and patient survival rates. In the United States, the overall incidence has risen from 24.4 percent to 29.2 percent. The prevalence of PD has been continuously growing. Patients with PD are more likely to need a kidney transplant and have a decreased risk of acquiring DGF. Some PD patients are getting kidney transplants, and some of them acquire DGF following the donation. Previous research has raised concerns about the increased risk of peritonitis, wound infection, and other complications during the post transplantation period; however, there is no agreement on how long the PD catheter should be retained after transplantation or whether PD should be performed in DGF. The purpose of this study is to assess the results of these individuals and compare them to those who received Hemodialysis (HD) during DGF.
Methods
We conducted a retrospective review of all Kidney Transplant Recipients from November 2015 to April 2019. A total of 224 patients had DGF during the study period. Inclusion criteria were all adult patients who were on any form of dialysis, received kidney transplantation, and developed DGF. All patients received dexamethasone or methylprednisolone at the time of transplantation. Induction was performed using antithymocyte globulin, alemtuzumab, or basiliximab based on the patient’s immunological risk, cause of End-Stage Renal Disease (ESRD)
DGF was defined as the need for renal replacement therapy within the first week of kidney transplantation. Modalities included HD, PD, and continuous venovenous hemofiltration. Duration of DGF was defined as the time interval between the first and the last dialysis. Peritonitis was defined as peritoneal fluid total white cell count of at least 100/μl and >50% polymorphonuclear cells after 2-hour dwell of peritoneal fluid.
Graft failure was defined as the return to dialysis, re-transplantation, or death. Outcomes related to rejection included rejection episodes during the period of DGF, 3, 6, and 12 months post-transplantation. Complications such as BK or cytomegalovirus (CMV) viremia, peritonitis in PD patients, catheter-associated bacteremia in patients on HD via CVC (Central bacteremia in patients on HD via CVC (Central Venous Catheter), and those related to the surgical procedure were recorded.
Results
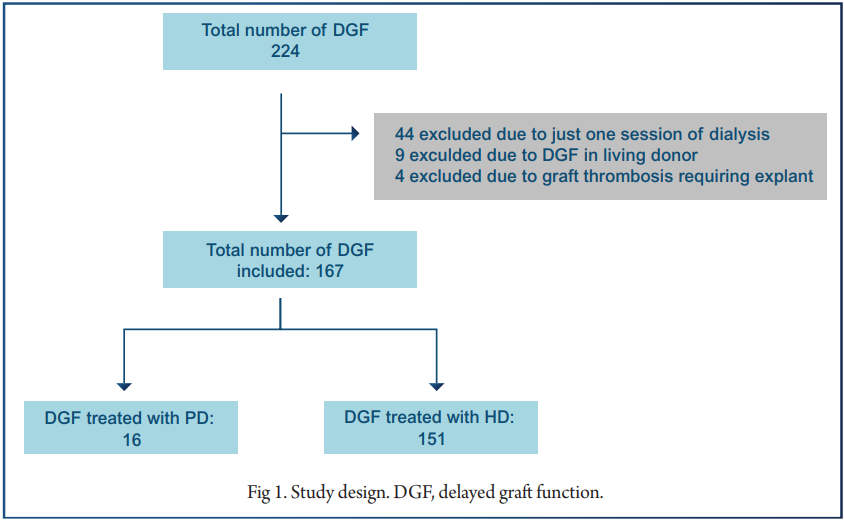
A total of 224 patients had DGF during the study period (Figure 1). One hundred sixty-seven patients fulfilled our selection criteria, of which 16 patients were in the PD and 151 were in the HD group. Fig 1 shows the study design.
Outcomes specific to DGF
There was no difference in the mean length of hospital stay post-transplantation between the two groups. Similarly, there was no difference in the mean duration of DGF between the two groups. In the PD group, 5 of 16 (31.3%) were switched to HD during the DGF period. Three were switched due to poor clearance, whereas one was switched due to pain which was related to peri-graft hematoma and another due to peritonitis. Only one patient (6.25%) had peritonitis, and none had a fluid leak or wound infection. Among the patients who underwent HD, 58 had a CVC placed. Two patients (3.4%) developed central line–associated bacteremia.
Rejection, Graft Survival, and Other Complications
The mean follow-up period was 27.8 ± 15.4 months for the PD group and 24.4 ± 12.3 months for the HD group. There was no statistically significant difference in serum creatinine and estimated glomerular filtration rate between the two groups at last follow-up. In addition, there was no difference in the total number of graft
Outcomes in All Pretransplantation PD Patients
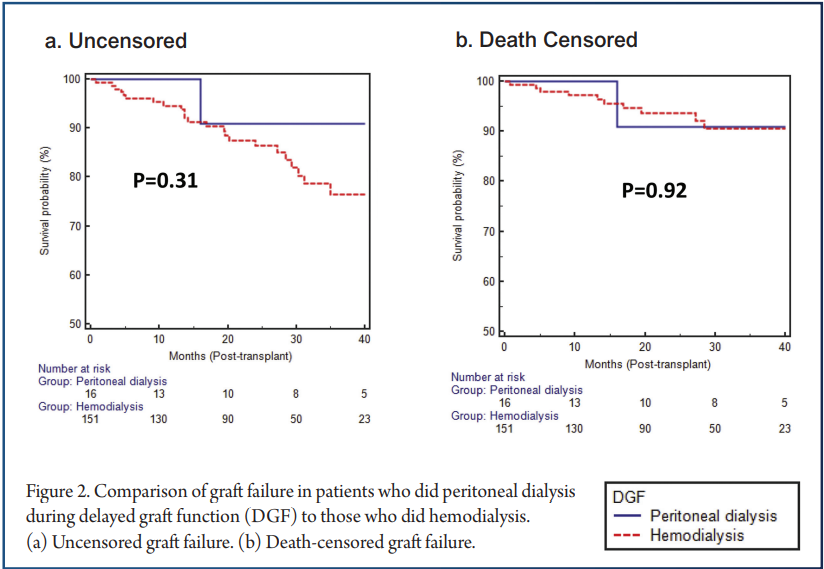
As opposed to HD patients, PD patients may have certain pretransplantation characteristics that affect the duration of DGF, particularly better residual renal function. Therefore, we separately analyzed the cohort of all pretransplantation PD patients who had DGF to see if switching the modality to HD had any effect on DGF failures (Figure 2a) or in death-censored graft failure (DCGFs) (Figure 2b) between the two groups. The rejection rates between the two groups were similar during the DGF period as well as in 3-, 6-, and 12-month periods.
Similarly, rates of CMV (cytomegalovirus) and BK infections and surgical complications did not differ significantly between the groups. duration. Of the 50 pretransplantation PD patients, 16 continued PD, whereas 34 were switched to HD. There was no difference in the duration of DGF between these two groups (8.6 ± 12.5 days for those who continued PD vs. 8.4 ± 8.9 days for those who switched to HD; P = 0.95). Similarly, there was no difference in the uncensored or DCGF in this subgroup of recipients with DGF.
Discussion
Individuals who received PD pretransplantation and continued it during DGF post-transplantation had similar outcomes to those who underwent HD during the DGF period in this group of 16 deceased donor kidney recipients. This includes both immediate DGF-related outcomes like hospital length of stay and DGF duration, as well as long-term outcomes like DCGF rate. In addition, consequences like rejections and infections were similar.
The increased risk of infections such as peritonitis and wound infections in individuals who get PD during DGF has been noted in earlier research. Although the use of high-dose immunosuppression in the initial post-transplantation period does raise the risk of infection, the hazards can be reduced with adequate PD technique and safeguards.
References
1. A. Siedlecki, W. Irish, D.C. Brennan Delayed graft function in the kidney transplant Am J Transplant, 11 (2011), pp. 2279-2296
2. B.J. Orandi, N.T. James, E.C. Hall, et al. Center-level variation in the development of delayed graft function after deceased donor kidney transplantatioTransplantation, 99 (2015), pp. 997-1002
3. D.E. Stewart, A.Y. Kucheryavaya, D.K. Kallsen, et al. Changes in deceased donor kidney transplantation one year after KAS implementation Am J Transplant, 16 (2016), pp. 1834-1847
4. T.J. Zens, J.S. Danobeitia, G. Leverson, et al. The impact of kidney donor profile index on delayed graft function and transplant outcomes: a single-center analysis Clin Transplant, 32 (2018), p. e13190
5. S.N. Tapiawala, K.J. Tinckam, C.J. Cardella, et al. Delayed graft function and the risk for death with a functioning graft J Am Soc Nephrol, 21 (2010), pp. 153-161
6. I. Quiroga, P. McShane, D.D. Koo, et al. Major effects of delayed graft function and cold ischaemia time on renal allograft survival Nephrol Dial Transplant, 21 (2006), pp. 1689-1696
7. N. Perico, D. Cattaneo, M.H. Sayegh, et al. Delayed graft function in kidney transplantation Lancet, 364 (2004), pp. 1814-1827
8. P. Buchanan, M. Schnitzler, D. Axelrod, et al. The clinical and financial burden of early dialysis after deceased donor kidney transplantation J Nephrol Therapeutic, S4 (2011), p. 001
9. United States Renal Data System 2018 USRDS annual data report: Epidemiology of kidney disease in the United States National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD (2018)
10.E. Lin, X.S. Cheng, K.K. Chin, et al. Home dialysis in the prospective payment system era J Am Soc Nephrol, 28 (2017), pp. 2993-3004
11.L.M. Moist, F.K. Port, S.M. Orzol, et al. Predictors of loss of residual renal function among new dialysis patients J Am Soc Nephrol, 11 (2000), pp. 556-564
12.M.A. Jansen, A.A. Hart, J.C. Korevaar, et al. NECOSAD Study Group: predictors of the rate of decline of residual renal function in incident dialysis patients Kidney Int, 62 (2002), pp. 1046-1053
13.J. Perl, R. Wald, P. McFarlane, et al. Hemodialysis vascular access modifies the association between dialysis modality and survival J Am Soc Nephrol, 22 (2011), pp. 1113-1121
14 .S. Wright, L. Wilson Quality of life and self-efficacy in three dialysis modalities: incenter hemodialysis, home hemodialysis, and home peritoneal dialysis Nephrol Nurs J, 42 (2015), pp. 463-476
15. J.J. Snyder, B.L. Kasiske, D.T. Gilbertson, et al. A comparison of transplant outcomes in peritoneal and hemodialysis patients Kidney Int, 62 (2002), pp. 1423-1430


