
Introduction
Cadmium exposure is linked to chronic kidney disease (CKD), however the best biomarker for detecting early cadmium-related nephrotoxicity in low-level exposure has yet to be identified. We used enzyme-linked immunosorbent assay (ELISA)-measured new renal biomarkers to determine the amount of renal impairment associated with cadmium burden in a cross-sectional study involving 167 CKD patients stratified by tertiles of urine cadmium levels (UCd). In non-dialysis-dependent CKD patients, urinary kidney injury molecule-1 (KIM-1) levels and age were the independent factors that were positively correlated with UCd after controlling for covariates (high vs. low UCd, odds ratio (95 percent confidence interval), 1.0016 (1.0001–1.0032), p = 0.043, and 1.0534 (1.0091–1.0997), p = 0.018). In the analyses, serum creatinine, estimated glomerular filtration rate, CKD staging, urine protein/creatinine ratio, urinary 8-hydroxy-2-deoxyguanosine (8-OHdG), and urinary epidermal growth factor (EGF) were not independently linked with UCd.
In conclusion, our findings suggest that urine KIM-1 levels determined by ELISA could be used as an early kidney damage marker in non-dialysis-dependent CKD patients exposed to low levels of cadmium. Furthermore, in this cohort, age was an independent factor that was positively linked with UCd.
Materials and Methods
The inclusion criteria were as follows:
(1) adult patients (≥20 years of age) with non-dialysis-dependent CKD stage 3a–5, and
(2) patients receiving follow-up treatment for at least one year in the nephrology outpatient department of the hospital.
Patients with a history of occupational or accidental heavy metal poisoning, liver cirrhosis, active infectious disease, malignancy under chemotherapy or radiotherapy, active alcoholism, or drug abuse were excluded. Blood biochemical data, including SCr, eGFR, hemoglobin, HbA1c, lipid profiles, liver enzymes, serum electrolytes, uric acid, and serum albumin were measured at the enrollment visit. The first-void urine in the morning was collected within one week after the enrollment visit for urinary renal biomarkers, including urinary protein/creatinine ratio (UPCR), urinary KIM-1, urinary 8-OHdG, and urinary EGF.
Results
Demographic, Clinical, and Biochemical Characteristics of Enrolled Patients
We enrolled 167 adult patients in this cross-sectional study, with 21.56 percent having CKD stage 3a, 27.54 percent having CKD stage 3b, 29.34 percent having CKD stage 4, and 21.56 percent having CKD stage 5. The most common comorbidities of the study population were hypertension (83.83%), followed by dyslipidemia (80.84%), gout or hyperuricemia (53.89%), diabetes (27.54%), vascular disease (21.56%), heart failure (10.18%), and COPD (8.98%). There were 13.17% of enrolled patients with a history of malignancy, with only a few patients having a history of transplantation (kidney transplant, 1.20%; extrarenal transplant, 1.20%). Of the enrolled patients, 40.72% received three or more types of antihypertensive agents. Additionally, 51.50% and 18.56% of the enrolled patients used lipid-lowering agents and glucose-lowering agents, respectively. The median eGFR was 28.80 mL/min/1.73 m2, and the median BMI was 25.04 kg/m2, while the median UCd was 3.43 μmol/g creatinine (IQR, 2.47–5.94 μmol/g creatinine).
Differences in Demographic, Clinical, and Biochemical Characteristics between Subclasses
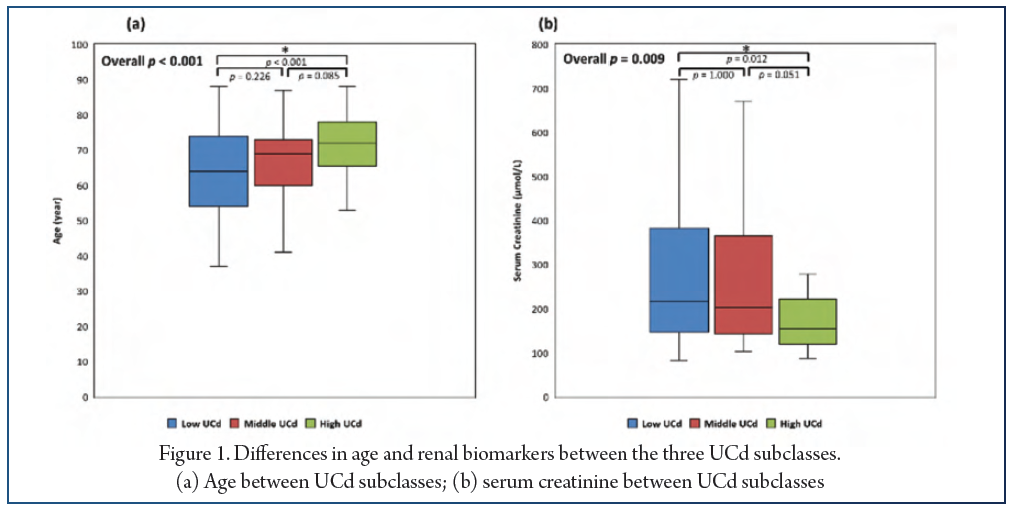
To analyze the UCd-associated factors of the study cohort with low-level cadmium exposure, we divided the enrolled patients into three subclasses based on the tertiles of UCd, namely, the low UCd (≤2.71 μmol/g creatinine, n = 55), the middle UCd (2.72–4.62 μmol/g creatinine, n = 55), and the high UCd (≥4.63 μmol/g creatinine, n = 57) subclasses. Furthermore, compared to the value of the low UCd subclass, the SCr value of the high UCd subclass was significantly lower (median (IQR), 215.70 (145.86–382.77), 202.44 (143.21–365.98), and 153.82 (120.22–221.88) μmol/L, respectively, p = 0.009) (Figure 1).
Differences in Urinary Renal Biomarkers between Subclasses
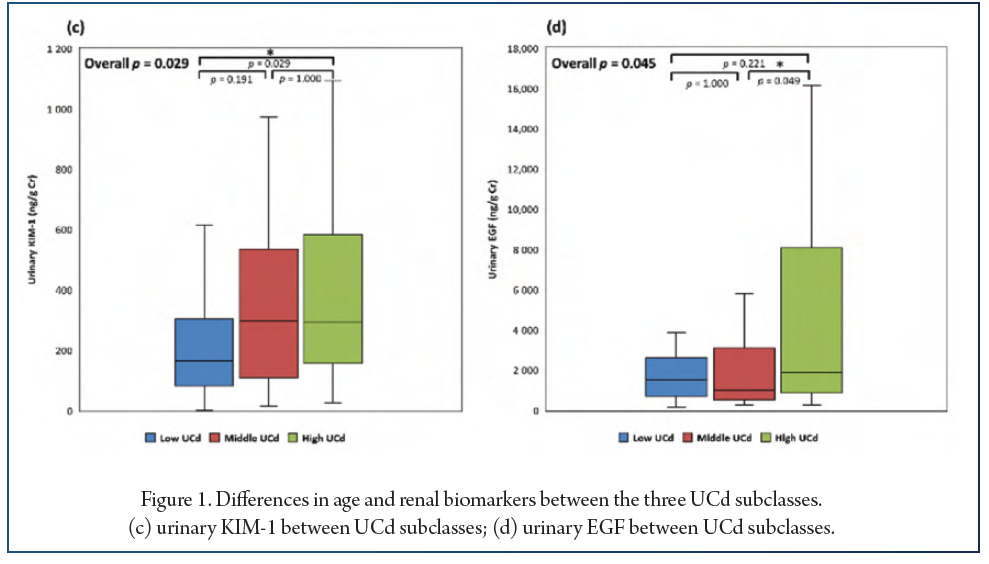
The profiles of urinary renal biomarkers were compared between the subclasses. The urinary KIM-1 levels of the high UCd subclass were higher than those of the low UCd subclass (median (IQR), 165.75 (82.18–304.43), 295.87 (108.03–535.65), and 292.42 (156.82–583.42) ng/g creatinine, p = 0.029). In addition, urinary EGF levels were higher in the high UCd subclass than in the middle UCd subclass (median (IQR), 1511.25 (701.96–2604.99), 981.26 (535.40–3114.03), and 1902.74 (868.00–8079.27) ng/g creatinine, p = 0.045) (Figure 1). On the other hand, UPCR and urinary 8-OHdG levels were not significantly different between the subclasses.
Factors and Renal Biomarkers Independently Associated with High UCd in CKD Patients
In the multinomial logistic regression analysis, after adjustment for age, smoking, diabetes, CKD staging, and covariates with a p-value ≤ 0.05 in univariate analyses, urinary KIM-1 level was an independent factor positively correlated with UCd in the CKD population (high vs. low UCd, odds ratio (95% confidence interval), 1.0016 (1.0001–1.0032), p = 0.043). Age was also positively associated with UCd after covariate adjustment (high vs. low UCd, odds ratio (95% confidence interval), 1.0534 (1.0091–1.0997), p = 0.018). On the other hand, the stage of CKD, SCr, and urinary EGF level were not significantly associated with UCd in the multivariate analyses.
Conclusions
In conclusion, our study indicated that ELISA-measured urinary KIM-1 levels were positively correlated with UCd in non-dialysis-dependent CKD patients even after adjustment for other covariates, which supports the use of urinary KIM-1 as an early renal injury marker in low-level cadmium exposure in this population. In addition, age was an independent factor positively associated with UCd in this population. Further studies are required to confirm these results.
References:
1. Genchi, G.; Sinicropi, M.S.; Lauria, G.; Carocci, A.; Catalano, A. The Effects of Cadmium Toxicity. Int. J. Environ. Res. Public Health 2020, 17, 3782.
2. Taha, M.M.; Mahdy-Abdallah, H.; Shahy, E.M.; Ibrahim, K.S.; Elserougy, S. Impact of occupational cadmium exposure on bone in sewage workers. Int. J. Occup. Environ. Health 2018, 24, 101–108.
3. Ginsberg, G.L. Cadmium Risk Assessment in Relation to Background Risk of Chronic Kidney Disease. J. Toxicol. Environ. Health Part A 2012, 75, 374–390.
4. Oh, C.-M.; Oh, I.-H.; Lee, J.-K.; Park, Y.H.; Choe, B.K.; Yoon, T.-Y.; Choi, J.-M. Blood cadmium levels are associated with a decline in lung function in males. Environ. Res. 2014, 132, 119–125.
5. Zhou, Z.; Lu, Y.-H.; Pi, H.-F.; Gao, P.; Li, M.; Zhang, L.; Pei, L.-P.; Mei, X.; Liu, L.; Zhao, Q.; et al. Cadmium Exposure is Associated with the Prevalence of Dyslipid-emia. Cell. Physiol. Biochem. 2016, 40, 633–643.
6. Vallée, A.; Gabet, A.; Grave, C.; Blacher, J.; Olié, V. Associations between urinary cadmium levels, blood pressure, and hypertension: The ESTEBAN survey. Environ. Sci. Pollut. Res. 2020, 27, 10748–10756.
7. Kumar, S.; Sharma, A. Cadmium toxicity: Effects on human reproduction and fertility. Rev. Environ. Health 2019, 34, 327–338.
8. Chen, H.-L.; Fang, J.; Chang, C.-J.; Wu, T.-F.; Wang, I.-K.; Fu, J.-F.; Huang, Y.-C.; Yen, J.-S.; Weng, C.-H.; Yen, T.-H. Environmental Cadmium Exposure and Dental Indices in Orthodontic Patients. Health 2021, 9, 413.
9. Dix-Cooper, L.; Kosatsky, T. Blood mercury, lead and cadmium levels and determinants of exposure among newcomer South and East Asian women of reproductive age living in Vancouver, Canada. Sci. Total Environ. 2017, 619–620, 1409–1419.
10. Liu, T.-Y.; Hung, Y.-M.; Huang, W.-C.; Wu, M.-L.; Lin, S.-L. Do people from Taiwan have higher heavy metal levels than those from Western countries? Singap. Med. J. 2017, 58, 267–271.
11. Kim, N.H.; Hyun, Y.Y.; Lee, K.-B.; Chang, Y.; Rhu, S.; Oh, K.-H.; Ahn, C. Environmental Heavy Metal Exposure and Chronic Kidney Disease in the General Population. J. Korean Med. Sci. 2015, 30, 272–277.
12. Navas-Acien, A.; Tellez-Plaza, M.; Guallar, E.; Muntner, P.; Silbergeld, E.; Jaar, B.; Weaver, V. Blood Cadmium and Lead and Chronic Kidney Disease in US Adults: A Joint Analysis. Am. J. Epidemiol. 2009, 170, 1156–1164.
13. Satarug, S.; Gobe, G.C.; Vesey, D.A.; Phelps, K.R. Cadmium and Lead Exposure, Nephrotoxicity, and Mortality. Toxics 2020, 8, 86.
14. Järup, L.; Åkesson, A. Current status of cadmium as an environmental health problem. Toxicol. Appl. Pharmacol. 2009, 238, 201–208.
15. Vacchi-Suzzi, C.; Kruse, D.; Harrington, J.; Levine, K.; Meliker, J.R. Is Urinary Cadmium a Biomarker of Long-term Exposure in Humans? A Review. Curr. Environ. Health Rep. 2016, 3, 450–458.
16. Tsai, H.-J.; Hung, C.-H.; Wang, C.-W.; Tu, H.-P.; Li, C.-H.; Tsai, C.-C.; Lin, W.-Y.; Chen, S.-C.; Kuo, C.-H. Associations among Heavy Metals and Proteinuria and Chronic Kidney Disease. Diagnostics 2021, 11, 282.
17. Wu, C.-Y.; Wong, C.-S.; Chung, C.-J.; Wu, M.-Y.; Huang, Y.-L.; Ao, P.-L.; Lin, Y.-F.; Lin, Y.-C.; Shiue, H.-S.; Su, C.-T.; et al. The association between plasma selenium and chronic kidney disease related to lead, cadmium and arsenic exposure in a Taiwanese population. J. Hazard. Mater. 2019, 375, 224–232.


