
Background
There is a paucity of data on the prevalence, adequate timing, and outcome of solid organ transplantation after severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection and the kinetics of immunoglobulin G (IgG) antibodies in these patients.
Methods
SARS-CoV-2 antinucleocapsid (N) IgG and polymerase chain reaction via a nasopharyngeal swab were analyzed in all patients within 24 h before liver or kidney transplantation. Kinetics of IgG antibodies were analyzed and compared with an immunocompetent cohort.
Results
Between May 1, 2020, and March 18, 2021, 168 patients underwent liver or kidney transplantation in our center, of which 11 (6.54%) patients with a previous SARS-CoV-2 infection were identified. The median interval between SARS-CoV-2 infection and transplantation was 4.5 mo (range, 0.9–11). After a median posttransplant follow-up of 4.9 mo, 10 out of 11 patients were alive without clinical signs of viral shedding or recurrent or active infection. One patient without symptom resolution at time of transplantation died after combined liver-kidney transplantation. In 9 out of 11 patients with previously polymerase chain reaction-confirmed infection, SARS-CoV-2 anti-N and antispike (S) IgG were detectable at day of transplantation. Absolute levels of anti-N and anti-S IgG were positively correlated, declined over time in all patients, and were significantly lower compared with immunocompetent individuals. All patients remained anti-S IgG positive until the last posttransplant follow-up, whereas 3 patients became anti-N negative.
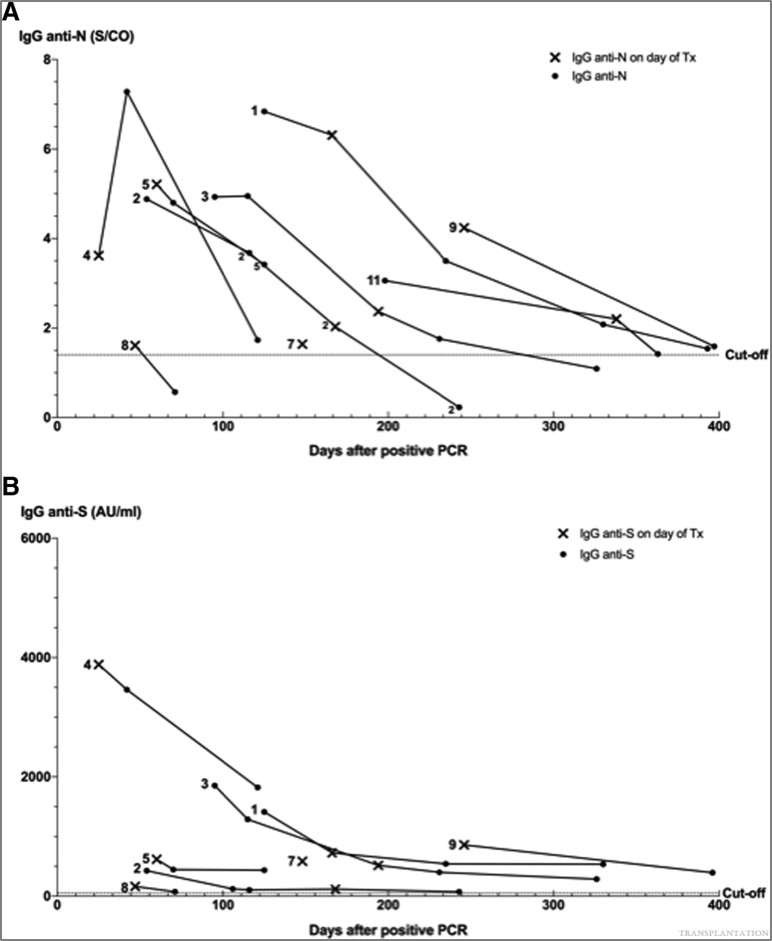
Kinetics of SARS-CoV-2 Anti-N and Anti-S IgG Antibodies and Comparison With Immunocompetent Cohort
The kinetics of SARS-CoV-2 anti-N and anti-S IgG antibodies are shown in Figures 1A and B, respectively. The median documented duration of IgG seropositivity was 168 d (range, 47–397) for anti-N and 196 d (range, 71–397) for anti-S IgG after positive PCR.
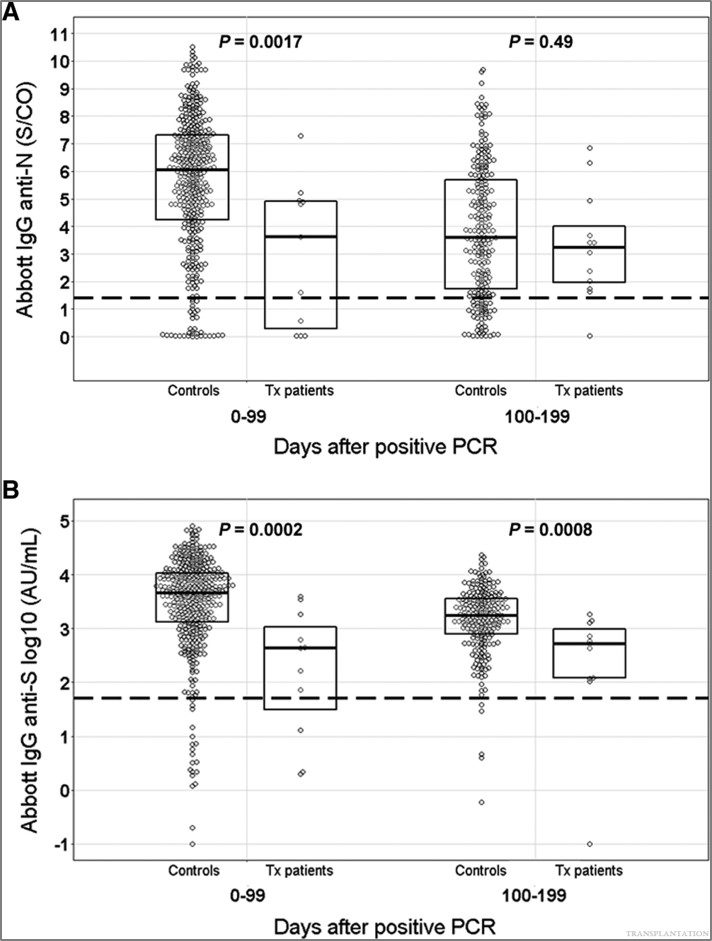
Absolute anti-S IgG levels were significantly lower in both the first 100 d (P = 0.0002) and 100 to 200 d (P = 0.0008) time periods after PCR positivity in our seroconverted transplant patients compared with immunocompetent individuals (Figure 2B), whereas anti-N IgG antibodies were only significantly lower in the first 100-d period (P = 0.0017) (Figure 2A).
Conclusions
We observed an uncomplicated course of liver or kidney transplantation after SARS-CoV-2 infection in selected patients. Although having lower absolute IgG antibody levels than immunocompetent individuals, all seroconverted patients remained anti-S IgG positive. These encouraging data need validation in larger studies.
References:
1. Iavarone M, D’Ambrosio R, Soria A, et al. High rates of 30-day mortality in patients with cirrhosis and COVID-19. J Hepatol. 2020;73:1063–1071.
2. Van Elslande J, Decru B, Jonckheere S, et al. Antibody response against SARS-CoV-2 spike protein and nucleoprotein evaluated by four automated immunoassays and three ELISAs. Clin Microbiol Infect. 2020;26:1557.e1–1557.e7.
3. Ravanan R, Callaghan CJ, Mumford L, et al. SARS-CoV-2 infection and early mortality of waitlisted and solid organ transplant recipients in England: a national cohort study. Am J Transplant. 2020;20:3008–3018.
4. American Association for the Study of Liver Diseases. COVID-19 and the liver. Available at https://www.aasld.org/about-aasld/covid-19-and-liver. Accessed April 17, 2021.
5. Khonsari RH, Bernaux M, Vie JJ, et al.; AP-HP/Universities/INSERM COVID-19 research collaboration, AP-HP COVID Clinical Data Warehouse initiative. Risks of early mortality and pulmonary complications following surgery in patients with COVID-19. Br J Surg. 2021;108:e158–e159.
6. Niess H, Börner N, Muenchhoff M, et al. Liver transplantation in a patient after COVID-19—rapid loss of antibodies and prolonged viral RNA shedding. Am J Transplant. 2021;21:1629–1632.
7. American Society of Transplantation. FAQs for organ transplantation. Available at https://www.myast.org/faqs-organ-transplantation. Accessed March 28, 2021.
8. The Transplantation Society. Guidance on coronavirus disease 2019 (COVID-19) for transplant clinicians. Available at https://tts.org/tid-about/tid-presidents-message/23-tid/tid-news/657-tid-update-and-guidance-on-2019-novel-coronavirus-2019-ncov-for-transplant-id-clinicians. Accessed April 27, 2021.
9. Di Maira T, Berenguer M. COVID-19 and liver transplantation. Nat Rev Gastroenterol Hepatol. 2020;17:526–528.
10. Kulkarni AV, Parthasarathy K, Kumar P, et al. Early liver transplantation after COVID-19 infection: the first report. Am J Transplant. 2021;21:2279–2284.
11. Van Elslande J, Oyaert M, Ailliet S, et al. Longitudinal follow-up of IgG anti-nucleocapsid antibodies in SARS-CoV-2 infected patients up to eight months after infection. J Clin Virol. 2021;136:104765.
12. Rouphael C, D’Amico G, Ricci K, et al. Successful orthotopic liver transplantation in a patient with a positive SARS-CoV2 test and acute liver failure secondary to acetaminophen overdose. Am J Transplant. 2021;21:1312–1316.
13. Martini S, Patrono D, Pittaluga F, et al. Urgent liver transplantation soon after recovery from COVID-19 in a patient with decompensated liver cirrhosis. Hepatol Commun. 2020;5:144–145.
14. Murad H, Dubberke E, Mattu M, et al. Repeat SARS-CoV-2 testing after recovery. Is a pretransplant PCR necessary? Am J Transplant. 2021;21:3206–3207.
15. Raveh Y, Simkins J, Nicolau-Raducu R. Liver transplantation in COVID-19 positive patients. Am J Transplant. 2021;21:1978.
16. Van Elslande J, Gruwier L, Godderis L, et al. Estimated half-life of SARS-CoV-2 anti-spike antibodies more than double the half-life of anti-nucleocapsid antibodies in healthcare workers. Clin Infect Dis. 2021;73:2366–2368.
17. Dhand A, Bodin R, Wolf DC, et al. Successful liver transplantation in a patient recovered from COVID-19. Transpl Infect Dis. 2021;23:e13492.
18. Raut V, Sonavane A, Shah K, et al. Successful liver transplantation immediately after recovery from COVID-19 in a highly endemic area. Transpl Int. 2021;34:376–377.
19. Varotti G, Dodi F, Garibotto G, et al. Successful kidney transplantation after COVID-19. Transpl Int. 2020;33:1333–1334.


