
Introduction
In patients with cirrhosis, the prevalence of renal dysfunction has been reported to range from 14 to 50 percent. Patients with cirrhosis and ascites are estimated to have a prevalence of 50 percent, while patients with advanced cirrhosis admitted to the hospital have a prevalence of 20 percent. The wide variation in prevalence is most likely due to different study populations and different definitions of renal failure. Renal replacement therapy may be required in patients with HRS who do not respond to medical treatment or who have severe renal failure due to another cause. In many of these patients, a simultaneous liver kidney transplant (SLK) is required to improve their post-transplant outcomes.
The criteria for identifying patients who would benefit from SLK transplantation, on the other hand, are based on consensus and lack strong evidence to back them up. Over the last decade, the health-care system has evolved, and newer drugs are now available for the treatment of cirrhosis complications. We’re trying to figure out how it affects the course and outcome of acute kidney injury. A small percentage of the patients may also be taking antiviral drugs for hepatitis B and C. If these patients are admitted, they will be included in the study, and we will look at how this drug affects acute kidney injury and vice versa. As a result, the current study was carried out to investigate the clinical profile of patients with acute kidney injury in liver cirrhosis.
Objectives
To study clinical profile, etiological factors, comparison of the course of acute kidney injury in cirrhosis with different etiologies and to study the association of acute kidney injury and liver cirrhosis with respect to hospital stay and mortality.
Materials and Methods
A total of 86 patients selected by simple random sampling with liver cirrhosis with AKI were included in the study. Patients admitted to wards of tertiary care hospitals and diagnosed with liver cirrhosis who presented with AKI or developed AKI during a hospital stay, those above > 12 years and patient and/or relative willing to give consent were included in the study.
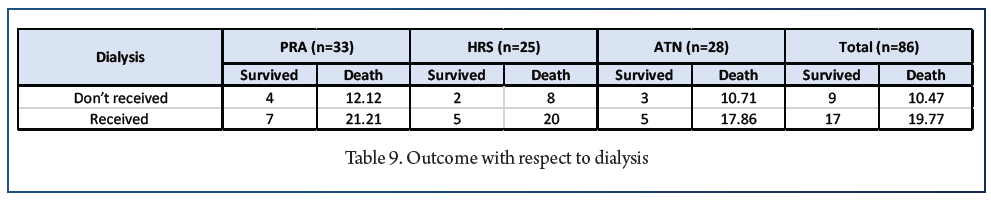
Results
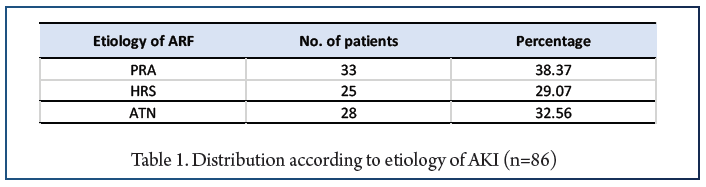
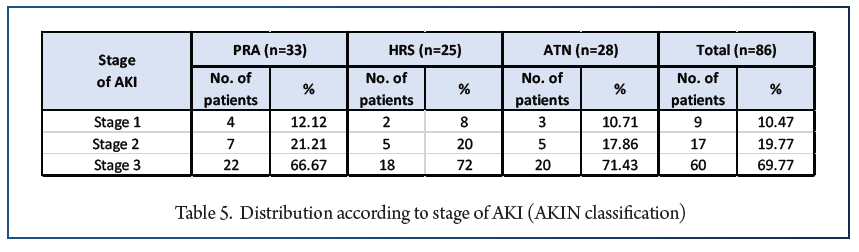
The difference observed between AKI due to PRA vs. HRS and PRA vs. ATN was statistically significant but the difference between HRS and ATN was not significant.
Conclusions
The occurrence of AKI in patients with liver cirrhosis is a common event associated with a worsening of the prognosis. This warrants special attention in the monitoring of the renal function in these patients. Using RIFLE/AKIN classification to detect AKI and determine its severity could allow earlier diagnosis of AKI and adaptation of its treatment according to the level of severity. Recognizing the common causes of AKI in cirrhosis along with early diagnosis and treatment is imperative for improving outcomes.
References:
1. D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44:217-231.
2. Du Cheyron D, Bouchet B, Parienti JJ, Ramakers M, Charbonneau P. The attributable mortality of acute renal failure in critically ill patients with liver cirrhosis. Intensive Care. Med. 2005;31:1693-1699.
3. Montoliu S, Ballesté B, Planas R, Alvarez MA, Rivera M, Miquel M et al. Incidence and prognosis of different types of functional renal failure in cirrhotic patients with ascites. Clin. Gastroenterol Hepatol. 2010;8:616-622.
4. Wu CC, Yeung LK, Tsai WS, Tseng CF, Chu P, Huang TY, et al. Incidence and factors predictive of acute renal failure in patients with advanced liver cirrhosis. Clin. Nephrol. 2006;65:28-33.
5. Angeli P, Ginès P, Wong F, Bernardi M, Boyer TD, Gerbes A, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: Revised consensus recommendations of the International Club of Ascites. J Hepatol. 2015;62:968-974.
6. Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology. 2008;48:2064-2077.
7. Ginès P, Schrier RW. Renal failure in cirrhosis. N Engl J Med. 2009;361:1279-1290.
8. Mehta RL, Kellum JA, Shah SV, et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit. Care. 2007;11: R31.
9. Wong F, Nadim MK, Kellum JA, Salerno F, Bellomo R, Gerbes A, et al. Working Party proposal for a revised classification system of renal dysfunction in patients with cirrhosis. Gut. 2011;60:702-709.
10. Caregaro L, Menon F, Angeli P, Amodio P, Merkel C, Bortoluzzi A, et al. Limitations of serum creatinine level and creatinine clearance as filtration markers in cirrhosis. Arch Intern Med. 1994;154:201-205.


