Introduction
Intra-patient variability (IPV) in tacrolimus blood concentrations has emerged as a potential biomarker for managing organ transplant patients. This study explored the relationship between the time in therapeutic range (TTR) of tacrolimus and its role in preventing acute graft-versus-host disease (GVHD) in patients undergoing allogeneic hematopoietic stem cell transplantation (HSCT). Patients were categorized based on GVHD severity, and their TTR during the first 4 weeks post-transplantation was analyzed. Findings revealed that patients with lower TTR had a higher risk of developing severe GVHD (Grade II–III), suggesting that maintaining stable tacrolimus levels is crucial for effective GVHD prophylaxis.
Given the narrow therapeutic window and individual pharmacokinetic variations of tacrolimus, therapeutic drug monitoring is essential post-HSCT. This study highlights that a higher TTR in the early post-transplant period, particularly within the first 4 weeks, may significantly reduce GVHD severity. These findings provide a new perspective on tacrolimus management, reinforcing the importance of optimizing blood concentration levels to improve HSCT outcomes. Establishing TTR as a key monitoring parameter could enhance GVHD prevention strategies and overall transplant success.
Methods
Study Design and Setting
This single-center, retrospective observational cohort study included Japanese patients (≥18 years) undergoing allogeneic HSCT at the University of Miyazaki Hospital between April 2018 and October 2023. Patients received tacrolimus for GVHD prophylaxis, and data on demographics, transplantation conditions, laboratory results, drug history, tacrolimus blood levels, and acute GVHD symptoms up to 100 days post-transplantation were collected. Each transplantation episode was considered independently, including patients who underwent multiple transplants. The study followed the Declaration of Helsinki guidelines and was approved by the University of Miyazaki Ethics Review Committee, which waived the need for informed consent due to its retrospective nature.
Tacrolimus Dosing and Variables
Tacrolimus was started via continuous IV infusion (0.02–0.03 mg/kg/day) a day before transplantation, with variations based on prophylaxis protocols. When used with PTCy, tacrolimus was initiated on day 5 post-transplant. MMF or methotrexate was administered alongside tacrolimus, with dosing adjusted per protocol. Blood tacrolimus concentrations were monitored using the ARCHITECT i1000SR system. The Rosendaal linear interpolation method calculated TTR using two therapeutic thresholds (≥10 ng/mL and ≥12 ng/mL) over three evaluation periods (2, 4, and 8 weeks). GVHD severity and organ involvement were recorded based on Japanese transplant guidelines.
Statistical Methods
Patients were grouped by acute GVHD severity (Grade 0–I vs. Grade II–III) and compared for baseline characteristics and tacrolimus TTR. Fisher’s exact test and the Mann–Whitney U test analyzed categorical and continuous variables. Receiver operating characteristic analysis identified TTR cut-off values linked to severe GVHD risk. Propensity score matching (PSM) minimized confounding effects using logistic regression, considering GVHD prophylaxis type and onset timing. Post-matching analyses reassessed TTR associations with GVHD severity. Cumulative GVHD incidence was compared using the log-rank test. Statistical analyses were conducted in R v.4.3.2, with P < 0.05 considered significant.
Results
All episodes
Patient Characteristics
This study included 80 transplant episodes, with 69 classified as Grade 0–I and 11 as Grade II–III. No cases of Grade IV GVHD were observed at initial diagnosis. Patient characteristics, including sex, age, body weight, height, clinical lab data, GVHD prophylaxis, transplant conditions, and disease diagnosis, showed no significant differences between groups.
Non-malignant disease patients, like those with adrenoleukodystrophy, received the same conditioning regimen and GVHD prophylaxis as malignant disease patients, ensuring comparable GVHD risk. GVHD-affected organs (P < 0.001) and severity (P < 0.001) significantly differed due to GVHD grade grouping. GVHD onset occurred earlier in the Grade II–III group than in the Grade 0–I group (P = 0.032).
TTR of tacrolimus blood concentrations
When the therapeutic range was ≥10 ng/mL, TTR10 during the first 2 and 8 weeks post-transplantation showed no significant difference between groups. However, TTR10 in the first 4 weeks was significantly lower in the Grade II–III group than in the Grade 0–I group (P = 0.049). For the ≥12 ng/mL range, TTR12 did not differ significantly at any time.
Receiver operating characteristic analysis identified a TTR10 cut-off of 75.9% (AUC: 0.686; specificity: 0.884; sensitivity: 0.545) for predicting acute GVHD (Grade II–III) (Fig. 1A). Patients with TTR10 ≤75.9% had a significantly higher GVHD frequency (Fig. 1B, P = 0.003) and cumulative incidence (Fig. 2, P < 0.001) than those with TTR10 >75.9%.
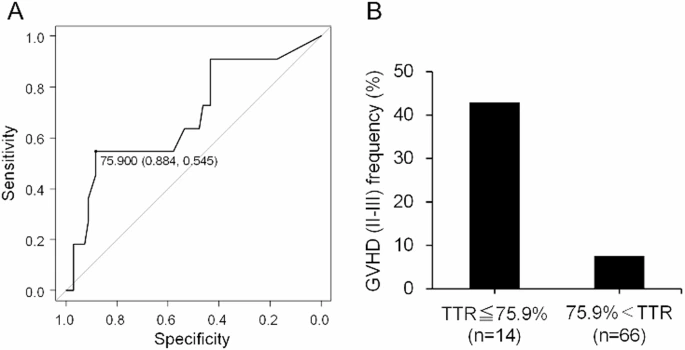
Figure 1.
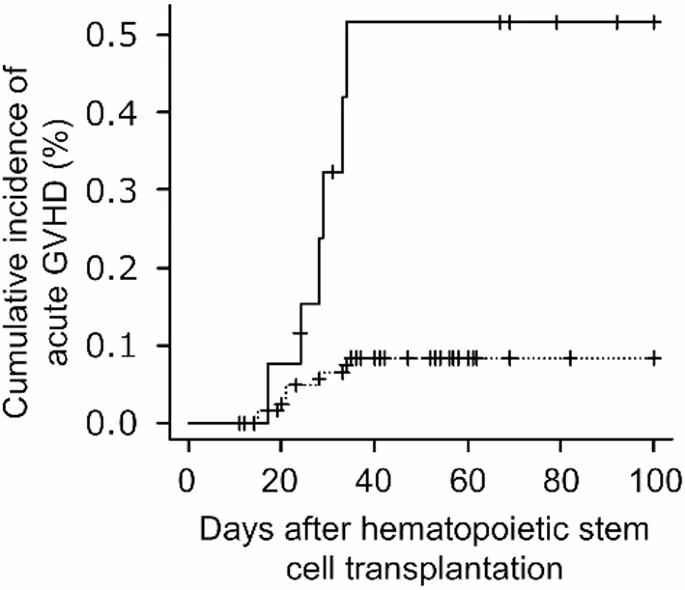
Figure 2.
Propensity score-matched episodes
Patient characteristics
Sixteen transplant episodes were analyzed, with an equal distribution of Grade 0–I and Grade II–III cases. Propensity scores were similar between groups (Supplementary Fig. 1). Table 2 shows no significant differences in patient demographics, clinical data, GVHD prophylaxis, transplant conditions, GVHD-developed organs, or days to GVHD onset (Supplementary Fig. 2). However, GVHD grades differed significantly (P < 0.001) due to the grouping criteria.
TTR of tacrolimus blood concentrations
With tacrolimus levels ≥10 ng/mL, TTR10 during the first 8 weeks post-transplantation showed no significant difference between groups (Table 2). However, TTR10 was significantly lower in the Grade II–III group during the first 2 (P = 0.043) and 4 weeks (P = 0.044). At ≥12 ng/mL, TTR12 showed no significant difference at any time (Table 2). ROC analysis identified TTR10 cut-off values of 83.3% (Fig. 3A) and 89.7% (Fig. 4A) for predicting Grade II–III GVHD. PSM-based classification showed significantly higher GVHD incidence in groups with TTR ≤83.3% (Fig. 3B, P = 0.041) and ≤89.7% (Fig. 4B, P = 0.041).
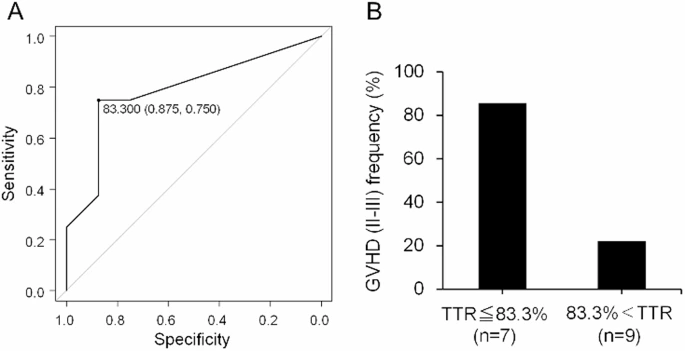
Figure 3.
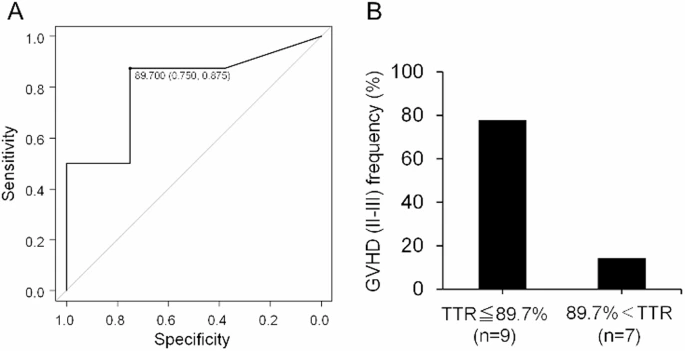
Figure 4.
Discussion
This study highlights the importance of maintaining a high Time in Therapeutic Range (TTR) of tacrolimus in preventing acute Graft-versus-Host Disease (GVHD) after Hematopoietic Stem Cell Transplantation (HSCT). Achieving a tacrolimus TTR of ≥10 nanograms per milliliter (TTR10) within the first four weeks post-transplantation significantly reduces the risk of severe GVHD, whereas maintaining a TTR of ≥12 nanograms per milliliter (TTR12) did not show additional benefits. Propensity Score Matching (PSM) analysis confirmed that lower TTR10 levels in the first two and four weeks increased GVHD risk. Additionally, elevated Tumor Necrosis Factor Alpha (TNFα) levels have been linked to GVHD onset, emphasizing the role of early TTR maintenance in suppressing T-cell activity. However, limitations include the single-center study design, lack of evaluation of upper tacrolimus limits, and absence of Human Leukocyte Antigen (HLA) concordance analysis. Furthermore, maintaining high tacrolimus levels post-GVHD onset may have influenced the findings. Frequent blood concentration monitoring is essential to minimize Intrapatient Variability (IPV) and keep levels within the therapeutic range, though the optimal measurement frequency requires further research to refine acute GVHD prophylaxis strategies.
References
1. Gooptu, M. & Antin, J. H. GVHD Prophylaxis 2020. Front. Immunol. 12, 605726 (2021).
2. Thomson, A. W., Bonham, C. A. & Zeevi, A. Mode of action of tacrolimus (FK506): molecular and cellular mechanisms. Ther. Drug Monit. 17, 584–591 (1995).
3. Plosker, G. L. & Foster, R. H. Tacrolimus: A further update of its pharmacology and therapeutic use in the management of organ transplantation. Drugs 59, 323–389 (2000).
4. Przepiorka, D. et al. Relationship of tacrolimus whole blood levels to efficacy and safety outcomes after unrelated donor marrow transplantation. Biol. Blood Marrow Transpl. 5, 94–97 (1999).
5. Gao, Y. & Ma, J. Tacrolimus in adult hematopoietic stem cell transplantation. Expert Opin. Drug Metab. Toxicol. 15, 803–811 (2019).
6. Kuypers, D. R. J. Intrapatient variability of Tacrolimus exposure in solid organ transplantation: a novel marker for clinical outcome. Clin. Pharmacol. Ther. 107, 347–358 (2020).
7. Yoshikawa, N. et al. Relationship between CYP3A5 polymorphism and Tacrolimus Blood concentration changes in allogeneic hematopoietic stem cell transplant recipients during continuous infusion. Pharmaceuticals (Basel). 14, 353 (2021).
8. Nakashima, T. et al. Differences in kinetics of tacrolimus concentration after letermovir discontinuation by type of concomitant azole antifungal. Int. J. Hematol. 115, 158–162 (2022).
9. Lao, Q. et al. Effect of Tacrolimus Time in Therapeutic Range on postoperative recurrence in patients undergoing liver transplantation for Liver Cancer. Ther. Drug Monit. 46, 42–48 (2024).
10. Adie, S. K. et al. Tacrolimus time in therapeutic range and long-term outcomes in heart transplant recipients. Pharmacotherapy 42, 106–111 (2022).