
Kidney transplantation remains the treatment of choice for end-stage renal failure. Despite several success stories, renal transplantation is fraught with the challenge of sensitisation as a result of which there are several instances of graft failure and rejection.
Sensitisation as a barrier to successful renal transplantation
Human Leucocyte Antigen (HLA) sensitisation poses a significant danger to successful kidney transplantation due to its deleterious impact before and after transplant – difficult crossmatch prior to transplant as well as an increased risk of acute and chronic antibody mediated rejection post transplantation. As such, HLA testing is pivotal in renal transplantation protocols. Desensitisation protocols help overcome this incompatibility and optimise the availability of compatible or acceptable donors.
Approaches to desensitization
Desensitisation protocols using novel immunomodulatory therapies together with better immunological risk stratification with sensitive DSA screening assays and avoidance techniques have resulted in improved transplantation rates as well as better transplantation outcomes. The approach to desensitisation is different in different patients and has been elucidated in the subsequent sections.
Desensitization strategies
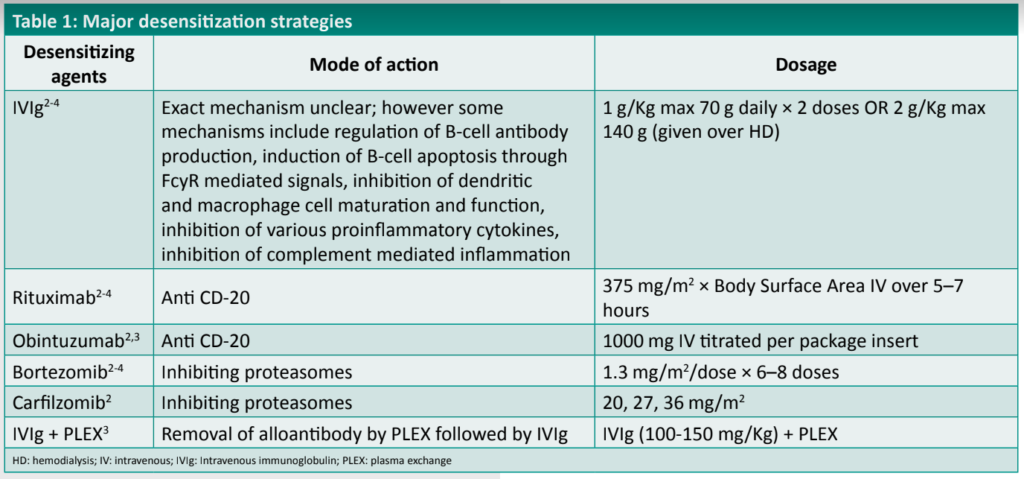
Some of the principal desensitization strategies have been outlined in Table 1.
Novel therapeutic approaches for kidney transplantation
Some of the other novel approaches to the achievement of desensitization for renal transplantation include those listed in Table 2.
Table 2: Novel therapeutic

The Complement Pathway as a mediator of renal allograft injury
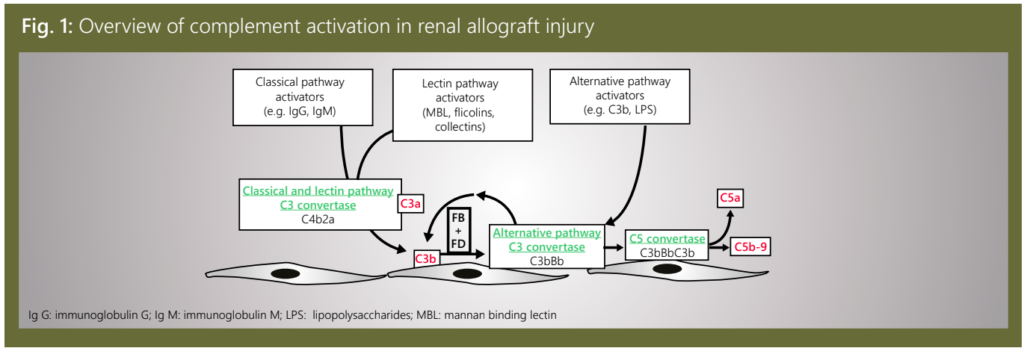
The complement system is activated through 3 distinct pathways: the classical pathway (CP), lectin pathway (LP), and alternative pathway (AP). These activation pathways involve different pathologic processes in the allograft, including donor brain death, I/R injury, and antibody mediated rejection.5
The CP is activated by antibodies bound to their target ligands. This may be particularly important in those transplant recipients with donor specific antibodies (DSA) reactive to polymorphic human leukocyte antigens (HLA) expressed on endothelial cells of the allograft. The LP is activated when activating proteins bind to sugars expressed on the surface of bacteria. LP activation can be initiated by several different proteins, including mannose binding lectin (MBL), collectins-10 and−11 (and, maybe, collectin-12), and ficolins 1–3. On the other hand, the AP is continuously and non-specifically activated in plasma through a process called “tick-over” whereby circulating C3 molecules are hydrolyzed to generate a form of C [C3(H2O)] that can combine with factor B and form a C3 convertase (i.e., an enzyme that cleaves additional C3 molecules).5
The mechanism by which the complement pathway plays a role in mediating renal allograft injury5 have been illustrated in Figure 1.
The role of some of the individual components of the complement pathway have been illustrated in Table 3.
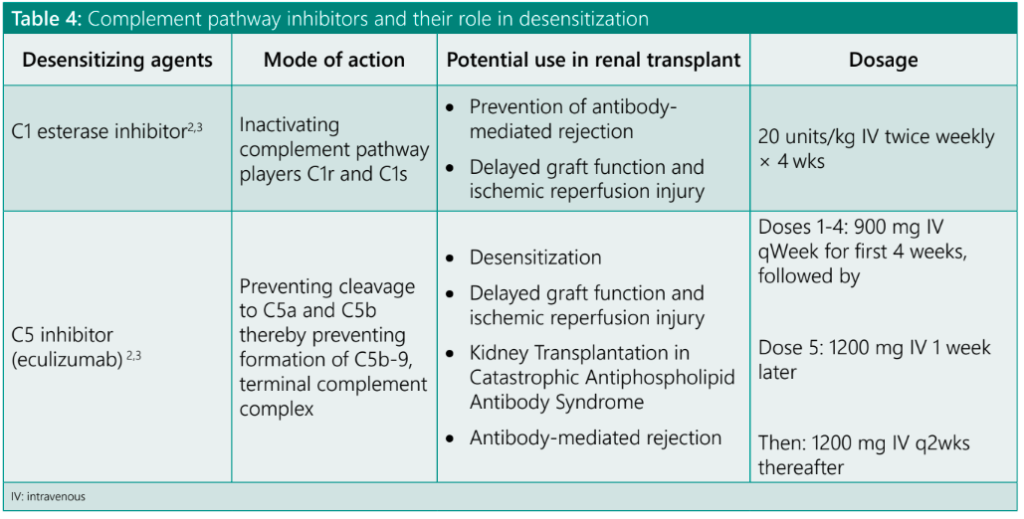
The role played by various complement pathway inhibitors in desensitization have been summarized in Table 4.
Summary and Conclusions
Renal transplantation remains the last resort for patients with renal failure and progressively worsening ESRD.
Sensitization poses a major challenge to the process of successful transplantation.
Desensitization, the approach to counter sensitization, with the help of advanced desensitization agents and protocols, has yielded better results in terms of less graft rejection and better survivorship outcomes.
While there are several novel therapeutic agents for desensitization, the agents inhibiting various components of the complement pathway have shown promising results across various clinical trials.
References
1. Alelign T, Ahmed MM, Bobosha K, et al. Kidney Transplantation: The Challenge of Human Leukocyte Antigen and Its Therapeutic Strategies. J Immunol Res. 2018;2018:5986740.
2. Sethi S, Choi J, Toyoda M, et al. Desensitization: Overcoming the Immunologic Barriers to Transplantation. J Immunol Res. 2017;2017: 6804678.
3. Wongsaroj P, Kahwaji J, Vo A, et al. Modern approaches to incompatible kidney transplantation. World J Nephrol. 2015;4(3):354–362.
4. Working Party of The British Transplantation Society. Guidelines for Antibody Incompatible Transplantation – 2016. Available at: https://bts.org.uk/wp-content/uploads/2016/09/02_BTS_Antibody_
Guidelines-1.pdf; Accessed on: Mar. 10, 2020.
5. Grafals M, Thurman JM. The Role of Complement in Organ Transplantation. Front. Immunol. 2019.
6. Nauser CL, Farrar CA, Sacks SH. Complement Recognition Pathways in Renal Transplantation. JASN. 2017;28(9):2571-2578.


