Introduction
Renal transplantation has become the most effective treatment for end-stage renal illness, although severe instances might result in renal allograft function loss owing to rejection and surgical complications. The prognosis of kidney transplant recipients will be greatly aided by early identification and diagnosis. Because ultrasound is a non-invasive examination that may offer information on the morphology and blood perfusion of the transplanted kidney while also indirectly reflecting the transplanted kidney’s condition, it has become the most often utilized monitoring tool following kidney transplantation.
B-mode ultrasound, colour Doppler ultrasound, and three-dimensional ultrasound are the most used diagnostic and monitoring techniques for kidney transplant recipients at the moment. The most frequent method for measuring resistance index (RI) is colour Doppler ultrasound. Although RI aids in the detection of acute renal insufficiency, it can’t distinguish between the causes of renal insufficiencies, such as acute rejection (AR), chronic allograft dysfunction (CAD), and graft renal artery stenosis (TRAS).
Contrast-enhanced ultrasonography has gained popularity in recent years as a novel method for monitoring the transplanted kidney’s microcirculation perfusion quantitatively. In comparison to other imaging techniques, contrast-enhanced ultrasonography has been demonstrated to offer distinct benefits in monitoring acute rejection following kidney transplantation, giving a credible basis for clinical intervention. This article reviews the current status of and recent research on contrast-enhanced ultrasound in acute rejection after renal transplantation.
Pathological Classification and Manifestations of Acute Rejection (AR)
According to the Banff 2007 Classification of Renal Allograft Pathology, AR after kidney transplantation is divided into cell-mediated and antibody-mediated AR. Among them, cell-mediated AR is mainly manifested as a large degree of inflammatory cell infiltration, which can be divided into 5 levels: grades IA, IB, IIA, IIB, and III.
Antibody-mediated AR is mainly manifested as positive for CD4, positive anti-donor antibody in the circulation, and morphological evidence of acute tissue damage, which can be divided into grades I, II, and III. Microscopic changes can alter the gross morphology and blood perfusion of the transplanted kidney, which is the basis for the ultrasound assessment of transplant function.
B-mode Ultrasound
B-mode ultrasound has a specific value in discovering the rejection reaction by observing the transplanted kidney’s morphology. It can monitor the morphology, size, internal structure, and perinephric condition of the transplanted kidney.
When AR occurs after renal transplantation, the kidney appears full, the volume is enlarged, the renal parenchymal wall is thick, the echo is reduced, and the kidney contour is not smooth; in severe cases, the renal parenchymal echo is not uniformly distributed, and the renal pyramid is enlarged with edema. B-mode ultrasound can detect borderline lesions and subclinical acute rejection through parenchymal swelling.
When AR after renal transplantation occurs, there are no obvious clinical symptoms or changes in the hemodynamic transplant index, indicating that the renal pyramidal veins are swollen, which reached a sensitivity of 96.2%. However, B-mode ultrasound has difficulty distinguishing AR from acute tubular necrosis and other complications, lacking diagnostic specificity. Therefore, more sensitive indicators need to be discovered (Fig 1).

Color Doppler Ultrasound
Color Doppler ultrasound can observe the blood perfusion in the kidney. When acute rejection occurs, the blood flow distribution in the kidney is asymmetrical, the arcuate arteries have almost no blood flow signals, and the interlobular arteries show intermittent flashing. In terms of pulsed Doppler, the venous blood flow speed significantly increases during the AR period after renal transplantation for venous blood perfusion. This resulted in a higher peak velocity during the diastolic period and an “arterial-like” pulsation phenomenon.
The resistance index (RI) value has been an important research topic, and its utility in the ultrasound diagnosis of kidney transplantation is still controversial. In early research, it was believed that the increase in RI value had diagnostic significance for AR. But later studies found that the RI value was a non-specific indicator and was affected by a series of factors in the long-term prognosis of kidney transplant patients (Fig 2).

Three-dimensional Ultrasound
The calculated volume of three-dimensional ultrasound is not affected by the geometry and position of the organ. It can measure the organ’s size more accurately, which makes it a good supplement to two-dimensional ultrasound. The combination of three-dimensional color power angiography (3D-CPA) and three-dimensional vascular volume imaging can evaluate kidney transplantation’s blood perfusion. Wei et al found that the three-dimensional reconstruction of the kidney volume in patients with AR was significantly larger than that in the normal group. The results were similar to the comparison of the kidney volume before and after AR, suggesting that rejection is related to the increase in kidney volume.
Contrast-enhanced Ultrasound (CEUS)
CEUS can detect the blood flow of microcirculation perfusion of tissues and organs, improving the effectiveness of ultrasound diagnosis and may be a significant predictor of early AR after renal transplantation.
At present, the most widely used contrast agent is SonoVue (Bracco, Milan, Italy). SonoVue microbubbles do not pass through the capillary wall, and overflow into the interstitial space. Its hemodynamic changes are similar to red blood cells, with good stability. As a blood pool imaging agent, SonoVue microbubbles can reflect tissue microcirculation blood perfusion changes in real time. Unlike CT and MRI contrast agents, SonoVue microbubbles have no liver and kidney toxicity and are not metabolized by the kidneys, being excreted through breathing. According to reports, the incidence of life-threatening adverse reactions in use of SonoVue microbubbles is only 0.001%.
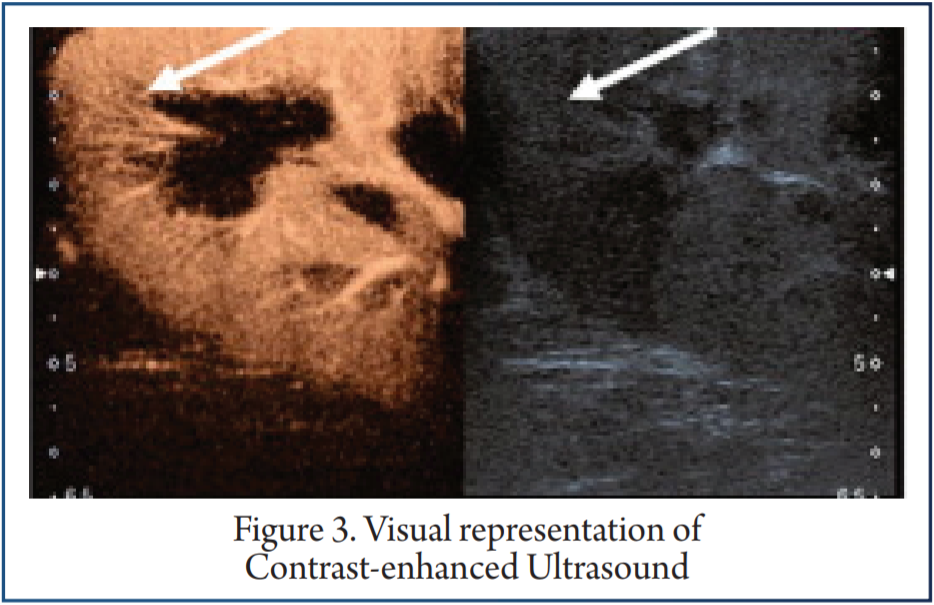
However, the safety and effectiveness of SonoVue have not been established in pregnant and lactating women, children, and adolescents. In most studies, the renal cortex and medulla are regarded as regions of interest. After acquiring the contrast image for about 2 minutes, the image analysis software is used to analyze the dynamic image generated by the contrast image and to generate the time-intensity curve (TIC) of the region of interest in the cortex and medulla of the kidney.
Multiple quantitative indicators, such as rise time (RT), time to peak (TTP), mean transit time (MTT), peak intensity (PI), and area under the ROC curve (AUC) are obtained. Comparing the differences in these indicators between different groups can assist in the differential diagnosis of kidney transplant complications (Fig 3).
Conclusion
Kidney transplantation is the terminal treatment for renal failure, and its functional status is crucial to the patient. Among the complications after kidney transplantation, acute rejection is still one of the main reasons for the poor short-term survival rate of patients.
Traditional two-dimensional ultrasound can observe the general morphological characteristics of transplantation, and color Doppler ultrasound can monitor the transplanted kidney’s intrarenal blood perfusion and measure blood flow parameters. However, these methods lack specificity and have limited value in the diagnosis of AR. Three-dimensional ultrasound measurements of the transplanted volume are more accurate than two-dimensional ultrasound and can obtain relevant blood vessel volume parameters, which provide a semi-quantitative index. CEUS is highly sensitive to blood perfusion. It has the advantages of being real-time and non-invasive, strong reproducibility, and non-nephrotoxic.
However, recent research on CEUS has mostly consisted of small-sample studies, case reports, or animal studies of kidney transplantation. Since the evaluation parameters are still in the preliminary stage in the differential diagnosis of complications, as a diagnostic tool, CEUS lacks sufficient specificity, and currently cannot replace the criterion standards for detection of AR after kidney transplantation, such as renal biopsy and CTA examination. With the advancement of instruments and the improvement of clinical diagnostic techniques, it is believed that CEUS can become the main diagnostic method for AR after kidney transplantation in the future.
References
1. Zhang Q, Yu Z, Xu Y, et al. Use of contrast-enhanced ultrasonography to evaluate chronic allograft nephropathy in rats and correlations between time-intensity curve parameters and allograft fibrosis. Ultrasound Med Biol. 2016;42(7):1574–83.
2. 2. Alvarez Rodriguez S, Hevia Palacios V, Sanz Mayayo E, et al. The usefulness of contrast-enhanced ultrasound in the assessment of early kidney transplant function and complications. Diagnostics (Basel) 2017;7(3):53.
3. Naesens M, Heylen L, Lerut E, et al. Intrarenal resistive index after renal transplantation. N Engl J Med. 2013;369(19):1797–806.
4. Korda D, Deak PA, Kozma V, et al. Role of contrast-enhanced ultrasound in the follow-up of kidney transplant patients. Transplant Proc. 2016;48(7):2544–47.
5. Granata A, Clementi S, Londrino F, et al. Renal transplant vascular complications: The role of Doppler ultrasound. J Ultrasound. 2015;18(2):101–7.
6. Cano H, Castaneda DA, Patino N, et al. Resistance index measured by Doppler ultrasound as a predictor of graft function after kidney transplantation. Transplant Proc. 2014;46(9):2972–74.
7. Zeisbrich M, Kihm LP, Druschler F, et al. When is contrast-enhanced sonography preferable over conventional ultrasound combined with Doppler imaging in renal transplantation? Clin Kidney J. 2015;8(5):606–14.
8. Solez K, Colvin RB, Racusen LC, et al. Banff 07 classification of renal allograft pathology: updates and future directions. Am J Transplant. 2008;8(4):753–60.
9. Gillard R, Milicevic M. Follow-up of kidney transplant by medical imaging techniques. Rev Med Liege. 2019;74(9):484–87.
10. Preuss S, Rother C, Renders L, et al. Sonography of the renal allograft: Correlation between doppler sonographic resistance index (RI) and histopathology. Clin Hemorheol Microcirc. 2018;70(4):413–22.
11. Krejci K, Zadrazil J, Tichy T, et al. Sonographic findings in borderline changes and subclinical acute renal allograft rejection. Eur J Radiol. 2009;71(2):288–95.
12. Gao BS, Wang YT, Wang G, et al. A more sensitive hallmark of acute rejection (AR) after renal transplantation: Color doppler ultrasonography of renal pyramids. Human Immunology. 2011;72(Suppl 1):S96.
13. Sutherland T, Temple F, Chang S, et al. Sonographic evaluation of renal transplant complications. J Med Imaging Radiat Oncol. 2010;54(3):211–18.
14. Drudi FM, Liberatore M, Cantisani V, et al. Role of color Doppler ultrasound in the evaluation of renal transplantation from living donors. J Ultrasound. 2014;17(3):207–13.
15. Imankulov S, Doskali M, Oskenbaeva K, et al. Evaluation of kidney allograft in the early posttransplant period using ultrasonography. Exp Clin Transplant. 2015;13(Suppl 3):62–65.
16. Wang HK, Chou YH, Yang AH, et al. Evaluation of cortical perfusion in renal transplants: Application of quantified power Doppler ultrasonography. Transplant Proc. 2008;40(7):2330–32.