Introduction
Only a few therapies have been identified as effective in preventing the advancement of chronic kidney disease (CKD) and the requirement for dialysis. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers were originally included on this restricted list, but it was recently broadened to include sodium/glucose cotransporter 2 (SGLT2) inhibitors.
In individuals with renal disease, these drugs also lower the risk of cardiovascular (CV) events. The hormone aldosterone has been linked to the development of heart failure. Inhibiting the effects of aldosterone with mineralocorticoid receptor antagonists (MRAs) reduces CV mortality and heart failure hospitalizations in patients with heart failure with lower ejection fraction and after myocardial infarction.
Because of its effects on endothelial activation, inflammation, and fibrosis, aldosterone is a possible mediator of kidney damage and a promising therapeutic target in diabetic kidney disease. Decades ago, salt-fed rats exposed to deoxycorticosterone suffered heart failure and nephrosclerosis, demonstrating the common link between mineralocorticoids, hearts, and kidneys. Later, animal studies showed that inhibiting deoxycorticosterone’s actions with an MRA minimised unfavourable CV and renal consequences.
The efficacy and safety of MRAs in preventing kidney failure and CV events in patients with CKD has generated attention, thanks to evidence from animal models and success in heart failure studies.
Method
In a Cochrane review summary in this issue of AJKD, Chung et al5 report an updated Cochrane systematic review and meta-analysis of 43 RCTs and quasi-RCTs with 5,279 patients (diabetic and nondiabetic) that compare MRAs to placebos or other antihypertensives in the setting of proteinuric CKD. Of particular note, only 2 RCTs with 2 events contributed to the estimate of treatment effects on kidney failure, and only 3 RCTs with 4 events contributed to the estimate of treatment effects on mortality.
To be fair, these trials were generally designed to inform the short-term effects of MRAs on laboratory parameters. The only outcomes with at least moderate certainty of an effect were for adverse effects including the increased risks of hyperkalemia, acute kidney injury, and gynecomastia.
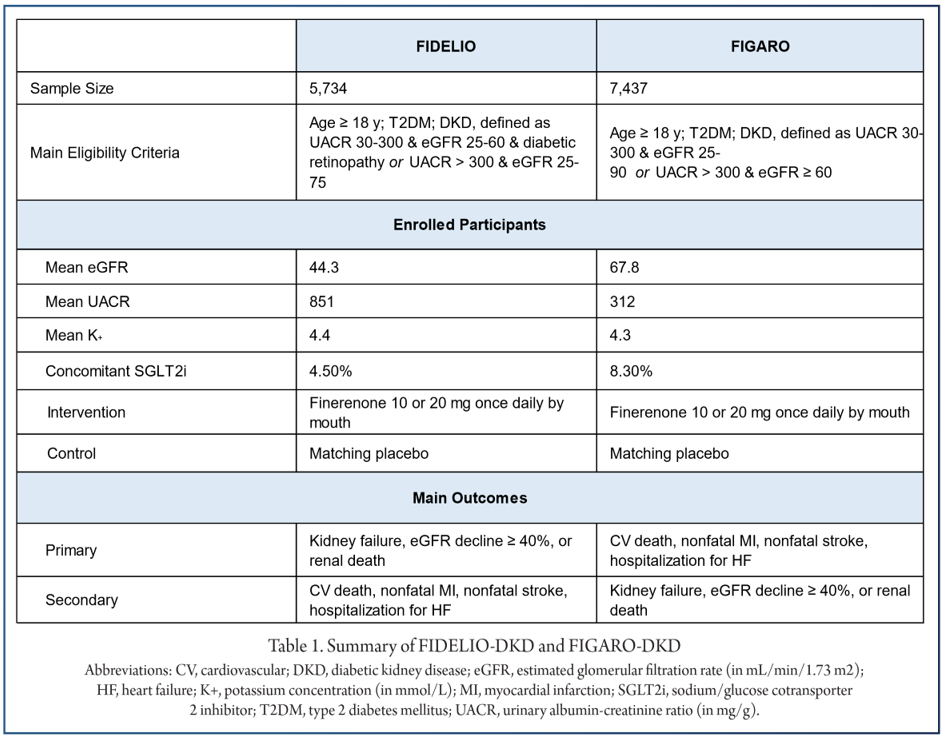
Despite the known adverse effects of MRAs, there remains hope of important kidney protective effects including attenuating loss of eGFR (mean difference, −3.00 [95% CI, −5.51 to −0.49] mL/min/1.73 m2 at a median 3.5 months’ follow-up) and reduced proteinuria (standardized mean difference, −0.51 [95% CI, −0.82 to −0.20]). The authors thus conclude that the evidence supporting MRAs in proteinuric CKD is uncertain. The review identified 2 ongoing RCTs (FIDELIO-DKD8 and FIGARO-DKD9) sponsored by Bayer. Both compare finerenone, at 10-20 mg orally per day, to placebo for the prevention of kidney failure and/or CV events. FIDELIO-DKD and FIGARO DKD are each as large as the entire systematic review’s population (Table 1) and are estimated to include approximately 1,000 primary outcome events each.
Conclusion
FIDELIO-DKD, which focuses on reducing major adverse kidney events in patients with diabetic kidney Recent RCTs and systematic reviews suggest promising disease, recently published their main results and treatment effects but, like the Cochrane Review for the demonstrated an approximate 18% relative risk reduceffects of MRAs in proteinuric CKD, the certainty of tion for the composite outcome of a ≥40% decline in beneficial effects is low owing to high risk of bias. eGFR, kidney failure, or renal death.
Additionally, finerenone resulted in an approximate 14% relative risk reduction in the main secondary outcome, a composite of CV death, nonfatal myocardial infarction, nonfatal stroke, or heart failure hospitalization.The even larger FIGARO-DKD trial focuses on the effects of finerenone on CV morbidity and mortality in patients with CKD and type 2 diabetes at high risk of CV events.
FIDELIO-DKD and FIGARO-DKD serve to remind the nephrology community that we should participate in and support the generation of high-quality evidence from such large trials so that we need not resign ourselves to decision making on the basis of low-certainty evidence.
References
1. Ezekowitz J.A. McAlister F.A. Aldosterone blockade and left ventricular dysfunction: a systematic review of randomized clinical trials. Eur Heart J. 2009; 30: 469-477
2. Selye H. Hall C.E. Rowley E.M. Malignant hypertension produced by treatment with desoxycorticosterone acetate and sodium chloride. Can Med Assoc J. 1943; 49:88-92
3. Kolkhof P. Delbeck M. Kretschmer A. et al. Finerenone, a novel selective nonsteroidal mineralocorticoid receptor antagonist protects from rat cardiorenal injury.
4. Blasi E.R. Rocha R. Rudolph A.E. Blomme E.A. Polly M.L. McMahon E.G.Aldosterone/salt induces renal inflammation and fibrosis in hypertensive rats.Kidney Int. 2003; 63: 1791-1800
5. Chung E.Y Strippoli G.F. Aldosterone antagonists in addition to renin agniotensin system antagonists for preventing the progression of CKD: editorial summary of a Cochrane review. Am J Kidney Dis. 2021; 77: 810-812
6. Bolignano D. Palmer S.C. Navaneethan S.D. Strippoli G.F. Aldosterone antagonists for preventing the progression of chronic kidney disease. Cochrane Database Syst Rev. 2014; 4: CD007004
7. Pyne L. Guyatt G.H. Walsh M. Change in albuminuria as a surrogate endpoint in chronic kidney disease. Lancet Diabetes Endocrinol. 2019; 7: 335
8. Bakris G.L. Agarwal R. Anker S.D. et al. Design and baseline characteristics of the Finerenone in Reducing Kidney Failure and Disease Progression in Diabetic Kidney Disease Trial. Am J Nephrol. 2019; 50: 333-344
9. Ruilope L.M. Agarwal R. Anker S.D. et al. Design and baseline characteristics of the Finerenone in Reducing Cardiovascular Mortality and Morbidity in Diabetic Kidney Disease Trial. Am J Nephrol. 2019; 50: 345-356
10. Bakris G.L. Agarwal R. Chan J.C. et al. Effect of finerenone on albuminuria in patients with diabetic nephropathy: a randomized clinical trial. JAMA. 2015; 314: 884-894
11. Bakris G.L. Agarwal R. Anker S.D. et al. FIDELIO-DKD Investigators Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020; 383: 2219-2229
12. McCullough K.P. Morgenstern H. Saran R. Herman W.H. Robinson B.M. Projecting ESRD incidence and prevalence in the United States through 2030. J Am Soc Nephrol. 2019; 30: 127-135