
Introduction
(Article introduction authored by Conquest Editorial Team)
Cognitive impairment is common in kidney failure patients, impacting their eligibility for kidney transplant (KT), quality of life, and survival. While cognitive function often improves post-KT, the extent and specific cognitive domains affected remain unclear.
Some brain changes like cerebral blood flow and neurochemical concentrations normalize after KT, but others, such as brain atrophy and white matter hyperintensities, may be permanent.
Systemic risk factors and immunosuppression, especially with tacrolimus, can also contribute to ongoing cognitive issues. Understanding which cognitive domains improve post-KT is crucial for assessing risks and determining the need for post-KT support. Prior studies on cognitive recovery after KT have been inconsistent and limited in scope, highlighting the need for larger studies with comprehensive neuropsychological assessments.
Methods
This single-center, prospective, longitudinal cohort study assessed cognitive function in kidney transplant (KT) candidates before and after KT.
Patients were enrolled while waiting for KT and followed for up to 12 months post-transplant. Cognitive function was measured using a battery of standard neuropsychological tests at baseline, 3 months, and 12 months after KT. If KT did not occur within a year, a second pre-KT assessment was conducted to maintain a time interval of less than one year. Longitudinal data from the National Alzheimer’s Coordination Center (NACC) were used for comparison to account for physiological changes and practice effects.
The study, approved by the University of Kansas Medical Center Institutional Review Board (IRB) and registered on clinicaltrials.gov (NCT01883349), used the same neuropsychological tests as NACC for comparison. Previous publications detailed brain alterations in this cohort before and after KT.
Participants and Data Collection
Adult patients on the KT waiting list expected to receive a KT within a year were included. Exclusion criteria included multiple-organ listing, recent stroke, uncontrolled psychosis, inability to speak or read English, active seizure disorder, or current antipsychotic medication use. Participants provided informed consent before starting.
Demographic data (age, race, sex, education) and clinical data (comorbidities, medication use, depression, smoking, primary cause of kidney failure, dialysis modality) were collected. Vital signs and laboratory data were recorded from medical records within 3 months of each visit.
Immunosuppression protocols, including induction (thymoglobulin or basiliximab, steroids, mycophenolate) and maintenance (tacrolimus, mycophenolate, and possibly low-dose prednisone), followed institutional practices and were not altered for the study.
Neurocognitive Testing
We used a battery of neuropsychological tests based on a broad review of the literature on memory and attention decline in kidney failure. These tests included assessment of global cognition with the Mini-Mental State Exam (MMSE),immediate and delayed episodic and declarative memory with Logical Memory I and II, psychomotor speed and visuospatial function with the Digit Symbol Substitution Test (DSST) and Trail Making Test (TMT) A, working memory and attention with Digit Span forward and backward, executive function with TMT B, and semantic memory, verbal fluency, and language with Category Fluency.
This battery takes approximately 2 hours to administer. Trained psychometricians or research personnel certified by trained psychometricians administered the neuropsychological tests in a private space that was designated for cognitive testing and was without distractions. Because acute illness can affect cognitive function, the study visit was rescheduled if a patient was not well.
Normative Cognitive Data
Normative cognitive data were obtained from the NACC Uniform Data Set, which includes standardized data from Alzheimer’s Disease Research Centers in the US. The dataset features 6,974 participants aged 24-75 years with normal cognition at enrollment. Data were collected annually before 2015, when some tests were replaced.
Statistical Analysis
Descriptive statistics were calculated for baseline characteristics. Categorical variables were analyzed using Pearson χ2 or Fisher exact tests, while continuous measurements were assessed with a 2-sample t-test. For longitudinal data, linear mixed models were used with random intercepts and fixed effects, including time as a continuous variable. Model assumptions were checked using quantile–quantile plots and residual analysis.
Logical Memory I and II and DSST scores were selected as primary outcomes, with a Bonferroni adjustment for statistical significance (0.017). Other tests, like MMSE and Category Fluency, were secondary outcomes with a significance level of 0.05. Linear mixed models assessed the impact of transplant status (normative, pre-KT, post-KT) on cognitive measures, adjusting for age, visits, sex, race, and education. Scatter plots were used to visualize cognitive changes over time and compare pre- and post-KT data with normative data. Regression lines were fitted and compared across different age groups. Analyses were conducted using R Studio and SAS software.
Results
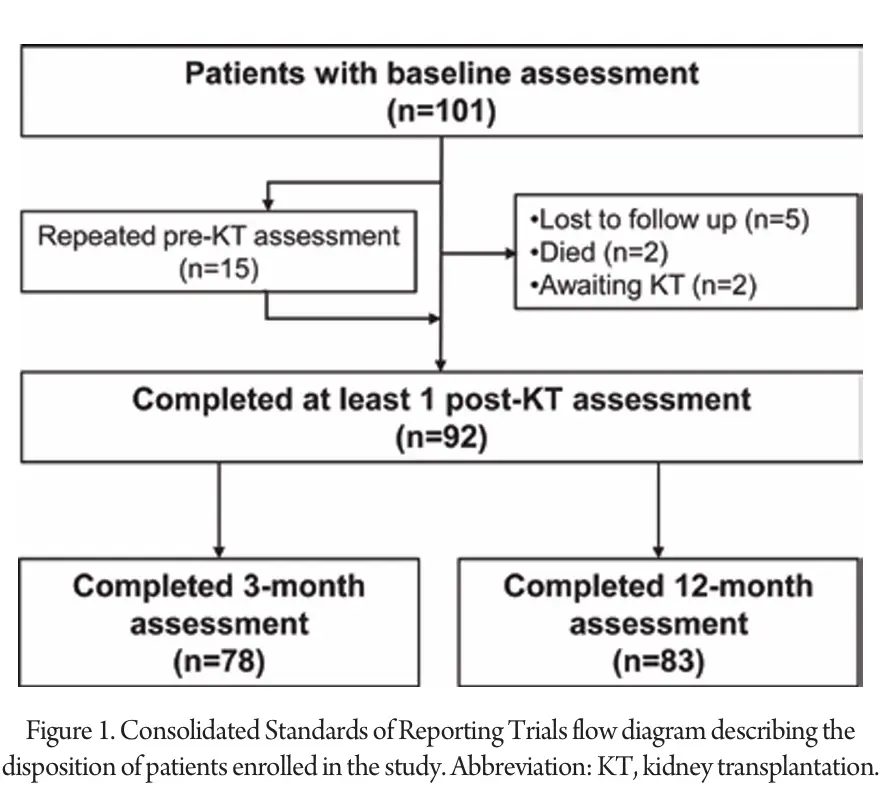
The leading causes of kidney failure were diabetes (25%) and autosomal-dominant polycystic kidney disease (17%). Of these, 15 patients did not receive a kidney transplant (KT) within a year and had repeat pre-KT cognitive assessments at that time (Table S1). Out of the 101 participants, 92 completed at least one post-KT assessment, with 78 completing the 3-month and 83 completing the 12-month assessments. Some missed visits, particularly the 3-month visit, due to the COVID-19 pandemic (Fig 1).
None of the patients received an ABO-incompatible KT. Most were given thymoglobulin induction with rapid steroid tapering, unless they had high rejection risk factors (e.g., previous transplants, high panel reactive antibody levels, Black race). Older patients (age >65) with lower rejection risk received basiliximab induction and continued maintenance prednisone.
The 9 patients without post-KT assessments did not differ from those who were assessed. KT-related clinical characteristics for the 92 patients with post-KT assessments are detailed in Table S3. Laboratory findings and vital signs at various time points are summarized in Table S4. After KT, all patients were on tacrolimus and had functional grafts.
Mean estimated glomerular filtration rates were 47.8 ± 14.9 mL/min at 3 months and 52.4 ± 16.6 mL/min at 1 year. Seven patients experienced delayed graft function and required dialysis post-KT, with a maximum delay of 1 month.
No participants were on dialysis during post-KT visits, and there were no allograft failures. Fourteen patients had cytomegalovirus infections, usually 4-9 months post-KT, following the discontinuation of prophylactic valacyclovir. Only 2 patients had acute rejection episodes, none within 1 month of a study visit.
Change in Cognitive Function
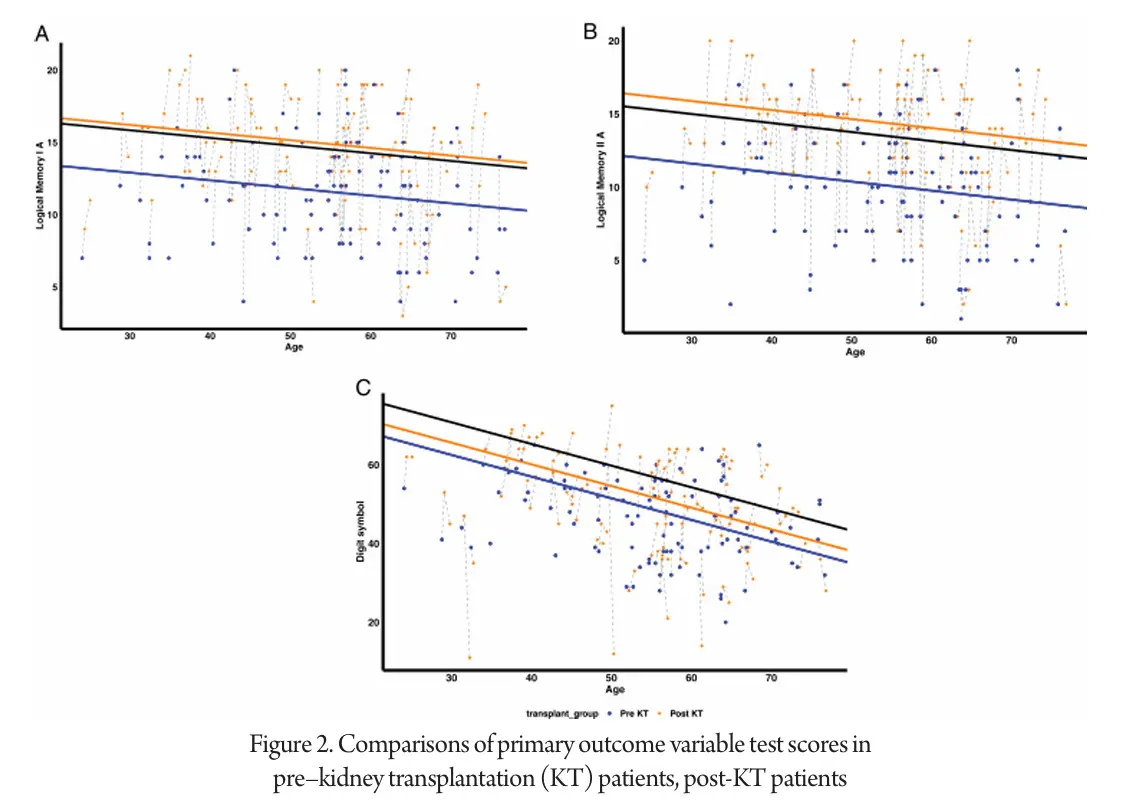
The average time to kidney transplant (KT) from the most recent cognitive assessment before KT was 105 days. Before KT, patients scored lower than the normative sample on tests such as Logical Memory I and II, DSST, Digit Span (backward), and Category Fluency (vegetables). After KT, improvements were observed in Logical Memory and DSST scores.
Figure 2 illustrates the comparisons of neuropsychological test scores before and after KT. Adjusted linear mixed model analysis revealed that pre-KT patients performed worse than normative data on most tests, including Logical Memory I and II, DSST, MMSE, Digit Span (backward), and Category Fluency (animals). Scores for Digit Span (forward) and Category Fluency (vegetables) were lower in pre-KT patients but not statistically significant. TMT A and B scores did not differ significantly from the normative data.
Discussion
In this study, we evaluated cognitive function in patients before and after kidney transplant (KT) using various neuropsychological tests. Our findings indicate that patients listed for KT exhibit cognitive impairments across several domains, including global cognition, episodic memory, and attention.
Post-KT, some cognitive domains, such as episodic and verbal declarative memory, showed significant improvement, while others, including semantic memory and psychomotor speed, demonstrated partial improvement. Notably, working memory, attention, and executive function did not improve significantly after KT. These varied results suggest that some cognitive impairments may be reversible, potentially related to metabolic changes, while others might be irreversible due to underlying conditions like cerebrovascular disease. The study highlights that cognitive improvements persisted for up to one year after KT and that episodic memory improvements could potentially enhance medical adherence.
Our study’s strengths include its longitudinal design, use of multiple neuropsychological tests, and adjustment for practice effects. However, limitations include its single-center nature and a demographic profile that may not fully represent the general kidney failure population. Overall, the study provides valuable insights into the cognitive benefits of KT and its implications for patient management.
References
1. A. Gupta, R.N. Montgomery, V. Bedros, et al. Subclinical cognitive impairment and listing for kidney transplantation Clin J Am Soc Nephrol, 14 (4) (2019), pp. 567-575,
2. A. Jurgensen, A.A. Qannus, A. Gupta Cognitive function in kidney transplantation Curr Transpl Rep, 7 (2020), pp. 145-153,
3. R.J. Lepping, R.N. Montgomery, P. Sharma, et al. Normalization of cerebral blood flow, neurochemicals, and white matter integrity after kidney transplantation J Am Soc Nephrol, 32 (1) (2021), p. 177,
4. A. Gupta, J.D. Mahnken, D.K. Johnson, et al. Prevalence and correlates of cognitive impairment in kidney transplant recipients BMC Nephrol, 18 (1) (2017), p. 158,
5. I. Mahaparn, R.J. Lepping, R.N. Montgomery, et al. The Association of tacrolimus formulation on cerebral blood flow and cognitive function Transplant Direct, 9 (8) (2023), Article e1511,
6. M. Kurella Tamura, V. Wadley, K. Yaffe, et al. Kidney function and cognitive impairment in US adults: the Reasons for Geographic and Racial Differences in Stroke (REGARDS) Study Am J Kidney Dis, 52 (2) (2008), pp. 227-234,
7. A. Gupta Cognitive function and kidney transplantation: putting current data into clinical perspective Kidney Med, 4 (12) (2022), Article 100566,
8. K. Griva, D. Thompson, D. Jayasena, A. Davenport, M. Harrison, S.P. Newman Cognitive functioning pre- to post-kidney transplantation–a prospective study Nephrol Dial Transplant, 21 (11) (2006), pp. 3275-3282,
9. J. Radic, D. Ljutic, M. Radic, V. Kovacic, K. Dodig-Curkovic, M. Sain Kidney transplantation improves cognitive and psychomotor functions in adult hemodialysis patients Am J Nephrol, 34 (5) (2011), pp. 399-406,
10. L. Kramer, C. Madl, F. Stockenhuber, et al. Beneficial effect of renal transplantation on cognitive brain function Kidney Int, 49 (3) (1996), pp. 833-838,
11. A. Gupta, R.J. Lepping, A.S. Yu, et al. Cognitive function and white matter changes associated with renal transplantation Am J Nephrol, 43 (1) (2016), pp. 50-57,
12. N.M. Chu, A.L. Gross, A.A. Shaffer, et al. Frailty and changes in cognitive function after kidney transplantation J Am Soc Nephrol, 30 (2) (2019), p. 336,
13. M.S. van Sandwijk, I.J.M. Ten Berge, M.W.A. Caan, et al. Cognitive improvement after kidney transplantation is associated with structural and functional changes on MRI Transplant Direct, 6 (3) (2020),
14. E. te Linde, C.J.M. van Roij, B.K.I. Meijers, H. De Loor, R.P.C. Kessels, J.F.M. Wetzels Cognitive function and uremic toxins after kidney transplantation: an exploratory study Kidney360, 1 (12) (2020), p. 1398,
15. A. Sharma, J. Yabes, Mawed S. Al, et al. Impact of cognitive function change on mortality in renal transplant and end-stage renal disease patients Am J Nephrol, 44 (6) (2016), pp. 462-472,


