Abstract
Hematopoietic cell transplantation (HCT) has significantly improved the prognosis for patients with severe aplastic anaemia (SAA); nonetheless, long-term morbidity, in particular the risk of subsequent malignancy, is still a major worry. The majority of the patients in earlier research looking into recurrent tumours following HCT had their organs transplanted due to a malignant condition. These investigations demonstrated that the most unfavourable risk factor is irradiation, whether it is administered as part of conditioning or as a pre-transplant treatment. As a result, SAA patients have been treated for decades using regimens that do not include total body radiation and include cyclophosphamide with or without antithymocyte globulin (ATG). The variability of the treatment modalities and/or the smaller cohort sizes of SAA patients have frequently made it difficult to identify additional risk factors for later malignancies.
Study
In this issue of Bone Marrow Transplantation, Phuong Vo et al. from the Fred Hutchinson Cancer Research Center analyzed subsequent cancers in 329 patients with SAA given HLA-matched related marrow grafts. The cohort was extremely homogenous in terms of conditioning regimen (cyclophosphamide ± ATG), source of hematopoietic stem cells (bone marrow) and prevention of graft-vs-host disease (GVHD) (metho- trexate ± cyclosporine), and the study covered a long follow-up with a median of 26 years (range 1–47). In this cohort the authors identified 53 cancers in 46 patients, 42 with solid tumors and 4 with blood cancers. They showed a cumulative incidence of subsequent cancers at 26 years of 11%, and 7% when non-melanoma skin cancers were excluded. Overall, there was a 2.03-fold excess of cancers when compared to a matched non-transplanted US population. Among them, tumors of the oropharyngeal cavity represented a remarkable proportion, being 13.63-fold higher than expected. The observed subsequent cancers had a late onset as nearly all developed between 14 and 34 years after HCT, and chronic GVHD was significantly associated with skin and oropharyngeal cancers (Fig. 1).
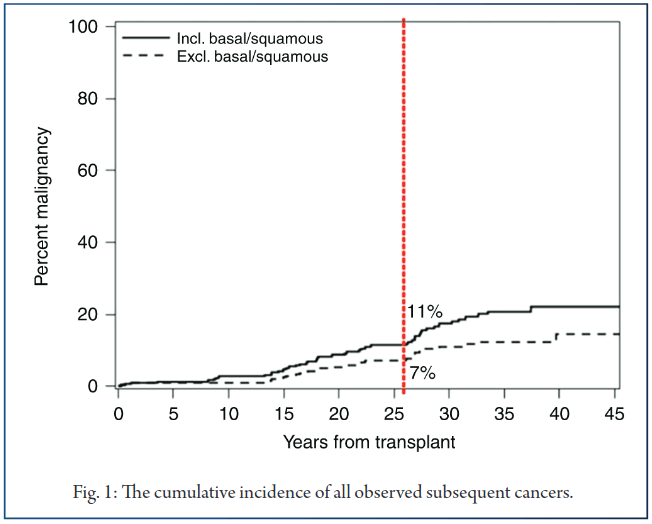
To improve the outcome of HCT, important changes have been attempted over the last decades, these modifications concern mainly the type of donor, stem cell source, conditioning regimen, and prevention of GVHD. the development of skin and oropharyngeal cancers, with an overall cumulative incidence of cancer at 26 years of 16.65% among patients with chronic GVHD, compared to 8.71% for patients without chronic GVHD. Although innovation is necessary, the interpretation of such changes may be particularly hazardous in rare diseases with small patients’ cohorts, as it is the case for SAA. This data shows that in addition to the deleterious effect of GVHD during the early phase of HCT, GVHD is also associated with late occurring subsequent cancers in SAA patients. The strengths of the present study are the homogeneity of the study cohort and the treatment strategy used over a remarkable long follow-up.
The results of this study show indeed only one thyroid cancer in the whole cohort, but there were 7 breast cancers in 139 transplanted females, thus showing a significant excess of observed breast cancers in relation to what was expected (SIR 2.50; p = 0.05). Indeed, the extreme consistency in using HLA-matched related donors, bone marrow as stem cell source and similar conditioning and GVHD prophylaxis over nearly 4 decades increases greatly the importance of the results. An important but not unexpected finding of this study was the negative prognostic value of chronic GVHD for These findings, suggesting that factors other than radiation would have an influence on the development of breast cancer, require confirmation in further cohorts and, if confirmed, the actual recommendations for long-term survivorship in respect of breast cancer risk should be accordingly adapted.
Secondly, the three factors which may potentially affect the immune system, i.e. GVHD prophylaxis with cyclo- sporine/methotrexate (compared to methotrexate alone), conditioning including ATG (compared to no ATG), as well as preceding immunosuppressive therapy (IST) before HCT were associated individually with a higher but not significant incidence of subsequent cancers. Another interesting finding is the donor type myelodysplastic syndromes (MDS) found in two patients. A defective marrow stromal/microenvironment has been described as a cofactor in the pathogenesis of SAA explaining partly the late evolution of a SAA treated with IST to a MDS. Finally, the late appearance of second cancers in SAA patients treated with HCT as well as the continuing appearance of cancers even 45 years after transplantation.
References:
1. Socie G, Henry-Amar M, Bacigalupo A, Hows J, Tichelli A, Ljungman P, et al. Malignant tumors occurring after treatment of aplastic anemia. European Bone Marrow Transplantation-Severe Aplastic Anaemia Working Party. N. Engl J Med. 1993;329:1152–7.
2. Curtis RE, Rowlings PA, Deeg HJ, Shriner DA, Socie G, Travis LB, et al. Solid cancers after bone marrow transplantation. N. Engl J Med. 1997;336:897–904.
3. Rizzo JD, Curtis RE, Socie G, Sobocinski KA, Gilbert E, Landgren O, et al. Solid cancers after allogeneic hematopoietic cell transplantation. Blood. 2009;113:1175–83.
4. Vo P, Onstad L, Flowers ME, Storb R. Cancers after HLA-matched related bone marrow transplantation for aplastic anemia. Bone Marrow Transplant. 2021.
5. NDePry JL, Vyas R, Lazarus HM, Caimi PF, Gerstenblith MR, Bordeaux JS. Cutaneous malignant neoplasms in hematopoietic cell transplant recipients: a systematic review. JAMA Dermatol. 2015;151:775–82.
6. Curtis RE, Metayer C, Rizzo JD, Socie G, Sobocinski KA, Flowers ME, et al. Impact of chronic GVHD therapy on the development of squamous-cell cancers after hematopoietic stem-cell transplantation: an international case-control study. Blood. 2005;105:3802–11.
7. Friedman DL, Rovo A, Leisenring W, Locasciulli A, Flowers ME, Tichelli A, et al. Increased risk of breast cancer among survivors of allogeneic hematopoietic cell transplantation: a report from the FHCRC and the EBMT-Late Effect Working Party. Blood. 2008;111:939–44.
8. Cohen A, Rovelli A, Merlo DF, van Lint MT, Lanino E, Bresters D, et al. Risk for secondary thyroid carcinoma after hematopoietic stem-cell transplantation: an EBMT Late Effects Working Party Study. J Clin Oncol: Off J Am Soc Clin Oncol. 2007;25:2449–54.
9. Majhail NS, Rizzo JD, Lee SJ, Aljurf M, Atsuta Y, Bonfim C, et al. Recommended screening and preventive practices for long-term survivors after hematopoietic cell transplantation. Bone Marrow Transplant. 2012;47:337–41.
10. Wiseman DH. Donor cell leukemia: a review. Biol Blood Marrow Transplant. 2011;17:771–89.
11. Passweg JR, Baldomero H, Basak GW, Chabannon C, Corbacioglu S, Duarte R, et al. The EBMT activity survey report 2017: a focus on allogeneic HCT for nonmalignant indications and on the use of non-HCT cell therapies. Bone marrow Transplant. 2019;54:1575–85.
12. Balderman SR, Calvi LM. Biology of BM failure syndromes: role of microenvironment and niches. Hematol Am Soc Hematol Educ Program. 2014;2014:71–6.