
Background and Objectives
Presently, both ABO-incompatible kidney transplantation (ABO-i KT) and ABO-compatible kidney transplantation (ABO-c KT) patients (adult and pediatric) have comparable outcomes as a result of advanced desensitization techniques and immunosuppressive therapy protocols. Yet, there exist unanswered questions as regards the type of ABO isoagglutinin — immunoglobulin M (IgM) or immunoglobulin M (IgG) — that is significantly involved in antibody-mediated rejection (AMR). This study aimed at investigating the outcomes of patients with high or low IgG isoagglutinin titers after employing the IgM titer as the surrogate target marker of plasma exchange and assessed the clinical significance of IgM and IgG anti- ABO antibodies in ABO-i KT.
Methodology
This retrospective study was carried out using the methodology outlined in Table 1.

Key Results
Comparison of outcomes
Survival outcomes were comparable in the two groups as depicted in Table 2.

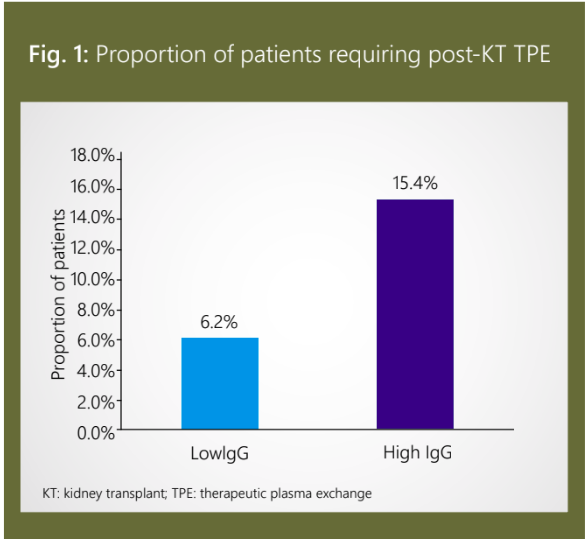
Compared to the low-IgG group, a larger number of patients in the high-IgG group required post- KT TPE due to a rebound in isoagglutinin titer as depicted in Figure 1.
AMR due to ABO antibody
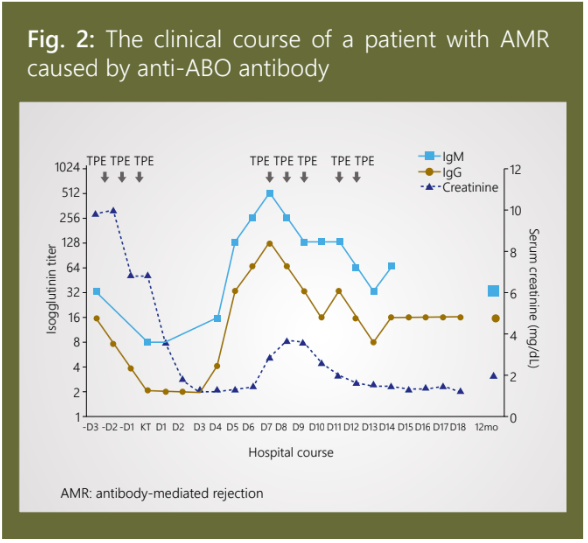
The clinical course that unfolded for the sole case of AMR (due to anti-ABO antibody) has been depicted in Figure 2.
Changes of IgM and IgG isoagglutinin titers
There was no between-group difference in the IgM isoagglutinin titers 3 months after renal transplantation. The IgG isoagglutinin titers of the high-IgG group continuously increased, in contrast with the titers of the low-IgG group, during the follow-up period. Even after 30 months, neither IgM nor IgG isoagglutinin titers reached their initial levels.
Conclusion
Patients with high pre-KT IgG isoagglutinin titers had equally successful outcomes as those with low IgG titers. ABO-i KT can be successfully performed by reducing the pre-KT IgM isoagglutinin titer to 4 or less, as determined by the immediate spin tube method.


