
Introduction
(Article introduction authored by Conquest Editorial Team)
Rheumatoid arthritis (RA) poses a diagnostic challenge due to its diverse clinical manifestations, ranging from polyarthritis to systemic complications. PET/CT imaging, particularly utilizing [18F]-FDG tracer, emerges as a promising adjunctive tool in the diagnostic landscape.
By capturing metabolic activity, PET/CT can unveil early inflammatory changes even before structural damage becomes evident on conventional imaging modalities. This capability holds significant potential for facilitating prompt and accurate diagnosis, enabling clinicians to initiate timely interventions and mitigate the risk of irreversible joint damage and systemic complications.
Moreover, PET/CT’s utility extends beyond diagnosis, encompassing the evaluation of therapeutic responses and prediction of RA remission. Its ability to provide a comprehensive assessment of disease activity throughout the body offers invaluable insights into treatment efficacy, enabling adjustments tailored to individual patient responses.
Additionally, by predicting the likelihood of remission, PET/CT empowers clinicians to optimize treatment strategies, fostering better outcomes and enhanced quality of life for patients grappling with this debilitating autoimmune condition. Nonetheless, while PET/CT represents a promising frontier in RA management, further research is imperative to validate its clinical utility and delineate standardized protocols for its integration into routine practice.
Evolving role of PET/CT in the evaluation of RA
PET was initially introduced in the 1970s primarily for diagnosing brain tumors. However, the accumulation of [18F]-fluorodeoxyglucose ([18F]-FDG) at sites of inflammation led to many false-positive oncological results.
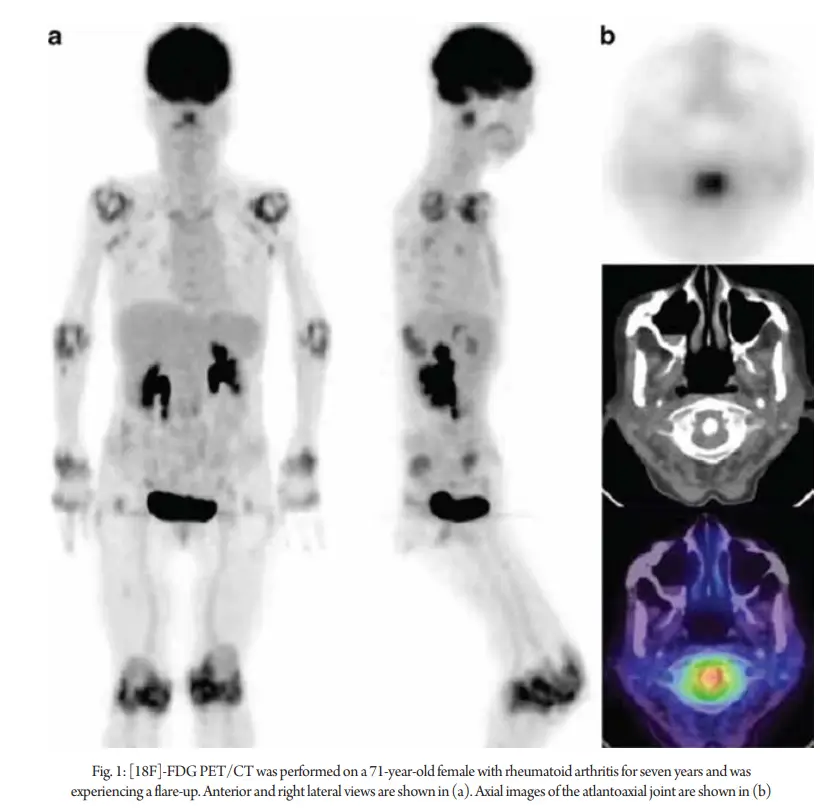
This increased uptake of [18F]-FDG now forms the basis for PET’s application in diagnosing and monitoring inflammatory disorders, including rheumatoid arthritis (RA) (Fig 1). When PET was combined with CT, it created a diagnostic modality that could identify both cellular metabolic information and anatomical details of organs.
In 1995, Palmar et al. reported the use of [18F]-FDG PET to quantify metabolic changes in RA. Subsequent studies have explored its potential for diagnosing, predicting disease progression, monitoring disease activity, and assessing therapeutic response. PET has been utilized to monitor inflammation in the myocardium and blood vessel walls, identifying subclinical risk factors for cardiac complications in RA.
Over 25 years, various PET parameters such as maximum standardized uptake value (SUVmax), metabolic tumor volume (MTV), and total lesion glycolysis (TLG), commonly used in cancer diagnosis, have been applied to study different conditions. In RA assessment, SUVmax has been primarily used to evaluate [18F]-FDG uptake at inflammation sites, albeit limited to subjectively defined regions of interest (ROI), emphasizing the need for a global disease score (GDS) to capture overall disease activity accurately.
Role of PET/CT in the evaluation of arthropathies in RA
PET/CT with [18F]-FDG and other radiotracers shows promise in evaluating arthropathies and excluding other differential diagnoses in rheumatoid arthritis (RA). Studies have utilized various PET parameters, including SUVmax and metabolic volume product, to differentiate RA from other arthropathies. Visual evaluation with the total visual score and the total number of PET-positive joints has demonstrated high sensitivity in clinical practice. Additionally, [18F]-NaF PET/CT has shown a strong positive correlation with disease activity in RA, aiding in accurate prediction of high disease activity. Moreover, PET/CT, employing tracers targeting biological pathways involved in angiogenesis and macrophage activity, offers insights into RA pathogenesis and treatment response. Tracers such as RGD and DPA-713 exhibit increased specificity and reduced background uptake, enhancing diagnostic accuracy. Furthermore, PET/CT plays a crucial role in distinguishing RA from polymyalgia rheumatica (PMR), with SUVmax being a valuable parameter in this differentiation. Recent systematic reviews and meta-analyses have further elucidated the diagnostic utility of [18F]-FDG PET/CT in PMR.
Role of PET/CT in the evaluation of systemic complications of RA
Another important use of PET/CT in RA is to diagnose complications. Complications of RA commonly include but are not limited to vasculitis, rheumatoid nodules, respiratory complications (pleuritis, pleural effusion, ILD), cardiovascular diseases (myocarditis, coronary artery disease, and heart failure), neurological, nephrological, ocular, and hematological complications. Notably, with the recent advent of PET/CT, it has become possible to diagnose or even predict future complications of RA.
Cardiovascular complications
Cardiovascular disease (CVD) is a leading cause of mortality in rheumatoid arthritis (RA), primarily due to vascular inflammation leading to atherosclerosis. [18F]-FDG PET/CT imaging has emerged as a valuable tool for assessing atherosclerosis and arterial wall inflammation in RA patients.
Studies have shown positive associations between PET parameters and CVD risk factors, with RA disease activity measured by DAS28-CRP also correlating with PET parameters. Additionally, [18F]-FDG PET/CT has been used to evaluate myocardial blood flow (MBF) and myocardial flow reserve (MFR) in RA patients, revealing lower MFR compared to controls, suggesting increased cardiovascular risk.
However, the predictive value of these findings for heart failure risk remains uncertain. Furthermore, [18F]-FDG PET/CT is increasingly utilized to diagnose and assess atherosclerosis, particularly revealing increased inflammation in the carotid arteries and aorta in RA patients compared to osteoarthritis patients.
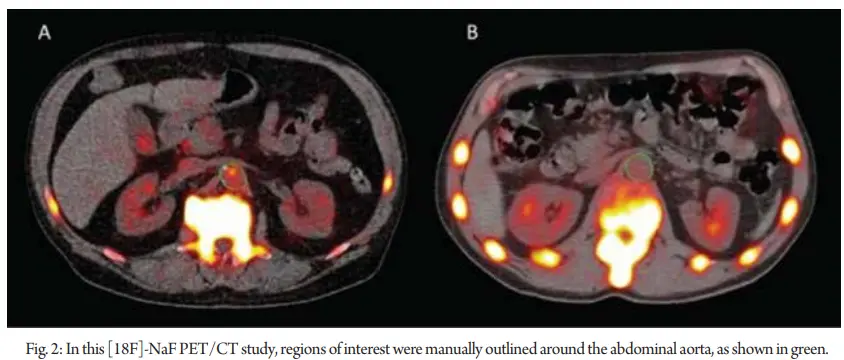
This heightened inflammation may contribute significantly to the elevated vascular complications observed in RA. Additionally, [18F]-NaF PET/CT has shown promise in identifying increased microcalcification in the abdominal aorta, predictive of atherosclerotic changes (Fig 2). However, [18F]-FDG PET/CT has limitations in detecting significant differences in microcalcifications between RA and healthy control groups.
Pulmonary complications
Rheumatoid arthritis (RA) can manifest in various pulmonary complications, including interstitial lung disease (ILD), pleural inflammation, airway involvement, and vasculitis-induced pulmonary hypertension. PET/CT imaging demonstrates its utility in detecting inflammatory changes in the pulmonary vasculature and lung parenchyma, ranging from nodules to ILD and resultant fibrosis.
Particularly, in distinguishing benign rheumatoid nodules from malignant ones, [18F]-FDG PET/CT has shown promise, as rheumatoid nodules exhibit relatively lower levels of [18F]-FDG avidity and do not coincide with [18F]-FDG-avid draining lymph nodes.
Additionally, [18F]-FDG uptake in normal-appearing lung parenchyma correlates with ILD severity, albeit lacking specificity.
Emerging research explores the potential of folate receptor (FR)-β as a radiotracer for imaging inflammatory conditions like RA, with [18F]-folate derivatives showing promise for future applications. Among these, 3′-Aza-2′-[18F]-fluoro-folic acid ([18F]-AzaFol) stands out as a novel radiotracer under development, offering potential advantages in RA imaging.
Role of PET/CT in monitoring treatment response in RA
Despite recent advancements, clinical assessment of treatment response in rheumatoid arthritis (RA) still typically requires a minimum of 12 weeks. [18F]-FDG PET can serve as a valuable tool for systemic monitoring of disease activity and treatment response.
Studies have demonstrated its efficacy in assessing response to various therapies, including tumor necrosis factor (TNF)-inhibitors, triple therapy, and rituximab.
For instance, changes in PET parameters such as SUVmean have been correlated with clinical disease activity indices and treatment outcomes.
Additionally, [18F]-FDG PET/CT has been utilized to evaluate the distribution and extent of joint involvement in different phases of the disease.
Furthermore, [18F]-FDG PET/CT has been employed to assess the efficacy of novel therapies such as tofacitinib, revealing suppressed disease activity and improved aortic inflammation following treatment.
These findings underscore the utility of [18F]-FDG PET/CT in therapeutic drug monitoring and assessing both synovial and aortic inflammation in RA patients.
In a study involving 64 rheumatoid arthritis (RA) patients treated with biologics for 6 months, [18F]-FDG PET/CT was utilized to assess inflammatory activity in the aortic walls.
Despite significant reductions in disease activity indices such as DAS28 and ESR, there was little change observed in [18F]-FDG uptake in the ascending aorta, indicating limited efficacy of biologics in preventing cardiovascular diseases.
However, conflicting results were observed in another study of 49 early RA cases treated with adalimumab, showing a favorable reduction in aortic wall inflammation after 6 months of treatment.
Moreover, [18F]-FDG PET/CT has been explored in predicting treatment outcomes, including tapering TNF-inhibitor (TNFi) therapy in RA patients with low disease activity.
Additionally, assessing joint-draining lymph nodes (LN) using whole-body [18F]-FDG PET/CT has shown promise in predicting the extent of joint inflammation and response to therapy in RA patients.
Changes in axillary LN metabolic activity were significantly correlated with clinical and laboratory parameters, suggesting its potential as an indicator of therapeutic response to biological therapy in RA.
Emerging evidence on the role of fibroblast activation protein inhibitor (FAPI) PET/CT in rheumatoid arthritis
Despite [18F]-FDG PET/CT’s utility in imaging inflammatory disorders like rheumatoid arthritis (RA), its limitations have spurred the search for alternative radiotracers with theranostic potential.
Fibroblast Activation Protein Inhibitor (FAPI) has emerged as a promising candidate due to its ability to target fibroblast-like synoviocytes (FLSs), crucial effector cells in inflamed joints of RA patients.
Studies have demonstrated the efficacy of FAPI radiotracers, such as [18F]AlF-NOTA-FAPI-04 and gallium-68 ([68Ga])-labeled FAP inhibitor, in imaging RA FLSs and evaluating joint disease activity.
Moreover, FAPI PET/CT shows promise in detecting pulmonary manifestations of RA, including lung fibrosis, and may aid in diagnosing seronegative RA, offering potential applications beyond conventional imaging modalities.
Furthermore, the theranostic potential of FAPI has been explored, with studies investigating FAP-targeted photodynamic treatment (FAP-tPDT) as a targeted therapy for RA.
Selective elimination of activated synovial fibroblasts expressing FAP shows promise as a therapeutic strategy, although further evidence is needed for clinical implementation.
Overall, FAPI PET/CT holds significant potential for both diagnostic imaging and targeted therapy in RA, offering new avenues for disease management.
Conclusion
PET/CT holds significant promise as an imaging tool for patients with rheumatoid arthritis (RA) and its complications. Studies utilizing PET/CT with various radiotracers such as [18F]-FDG, [18F]-NaF, FAPI, and others have demonstrated its utility in assessing disease activity, monitoring therapeutic response, escalating or tapering therapy, and identifying complications. PET/CT also plays a role in ruling out differential diagnoses like polymyalgia rheumatica (PMR). While newer radiotracers with potentially higher specificity for RA evaluation are being investigated, most are still in preclinical stages or involve small-scale studies with limited evidence.
PET/CT with [18F]-FDG and [18F]-NaF shows promise for early RA diagnosis and intervention to mitigate complications, but further research is needed before its routine clinical integration in managing RA.
1. Sparks JA. Rheumatoid arthritis. Ann Intern Med. 2019;170:C1–16. https://doi.org/10.7326/AITC201901010.
2. Arima H, Koirala S, Nema K, Nakano M, Ito H, Poudel KM, et al. High prevalence of rheumatoid arthritis and its risk factors among Tibetan highlanders living in Tsarang, Mustang district of Nepal. J Physiol Anthropol. 2022;41:12. https://doi.org/10.1186/s40101-022-00283-3.
3. Wasserman A. Rheumatoid arthritis: common questions about diagnosis and management. Am Fam Physician. 2018;97:455–62.
4. Sparks JA, Barbhaiya M, Tedeschi SK, Leatherwood CL, Tabung FK, Speyer CB, et al. Inflammatory dietary pattern and risk of developing rheumatoid arthritis in women. Clin Rheumatol. 2019;38:243–50. https://doi.org/10.1007/s10067-018-4261-5.
5. Dong H, Julien PJ, Demoruelle MK, Deane KD, Weisman MH. Interstitial lung abnormalities in patients with early rheumatoid arthritis: a pilot study evaluating prevalence and progression. Eur J Rheumatol Inflamm. 2019;6:193–8. https://doi.org/10.5152/eurjrheum.2019.19044.
6. Scherer HU, Häupl T, Burmester GR. The etiology of rheumatoid arthritis. J Autoimmun. 2020;110: 102400. https://doi.org/10.1016/j.jaut.2019.102400.
7. Lora V, Cerroni L, Cota C. Skin manifestations of rheumatoid arthritis. G Ital Dermatol Venereol. 2018;153:243–55. https://doi.org/10.23736/S0392-0488.18.05872-8.
8. Littlejohn EA, Monrad SU. Early diagnosis and treatment of rheumatoid arthritis. Prim Care. 2018;45:237–55. https://doi.org/10.1016/j.pop.2018.02.010.
9. Chen X, Zhang M, Wang T, Li Y, Wei M. Influence factors of extra-articular manifestations in rheumatoid arthritis. Open Med. 2020;15:787–95. https://doi.org/10.1515/med-2020-0217.
10. Smolen JS, Landewé R, Bijlsma J, Burmester G, Chatzidionysiou K, Dougados M, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis. 2017;76:960–77. https://doi.org/10.1136/annrheumdis-2016-210715.
11. Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review. JAMA. 2018;320:1360–72. https://doi.org/10.1001/jama.2018.13103.
12. Radu A-F, Bungau SG. Management of rheumatoid arthritis: an overview. Cells. 2021. https://doi.org/10.3390/cells10112857.
13. Fuchs HA, Kaye JJ, Callahan LF, Nance EP, Pincus T. Evidence of significant radiographic damage in rheumatoid arthritis within the first 2 years of disease. J Rheumatol. 1989;16:585–91.
14. van der Heijde DM, van Leeuwen MA, van Riel PL, Koster AM, van’t Hof MA, van Rijswijk MH, et al. Biannual radiographic assessments of hands and feet in a three-year prospective followup of patients with early rheumatoid arthritis. Arthritis Rheum. 1992;35:26–34. https://doi.org/10.1002/art.1780350105.
15. Ranganath VK, Hammer HB, McQueen FM. Contemporary imaging of rheumatoid arthritis: clinical role of ultrasound and MRI. Best Pract Res Clin Rheumatol. 2020;34: 101593. https://doi.org/10.1016/j.berh.2020.101593.
16. Armstrong TM, Grainger AJ, Rowbotham E. Imaging of rheumatological disorders. Magn Reson Imaging Clin N Am. 2023;31:309–20. https://doi.org/10.1016/j.mric.2023.01.008.
17. Bruijnen STG, Verweij NJF, Gent YYJ, Huisman MC, Windhorst AD, Kassiou M, et al. Imaging disease activity of rheumatoid arthritis by macrophage targeting using second generation translocator protein positron emission tomography tracers. PLoS ONE. 2019;14: e0222844. https://doi.org/10.1371/journal.pone.0222844.
18. Chaudhari AJ, Raynor WY, Gholamrezanezhad A, Werner TJ, Rajapakse CS, Alavi A. Total-body PET imaging of musculoskeletal disorders. PET Clin. 2021;16:99–117. https://doi.org/10.1016/j.cpet.2020.09.012.


