
Abstract
Failure of the allograft is a typical occurrence in kidney transplant patients. Complex management decisions are frequently required when a transplant fails, such as when and how to wean immunosuppression and begin the transition to a second transplant or to dialysis. These choices are taken in light of significant worries about conflicting dangers, such as infection and sensitization. Unfortunately, practise patterns are inconsistent and inadequate given that patients with failed allografts face extra morbidity and mortality compared to their transplant-naive counterparts since the care of the failed allograft is currently guided by very poor-quality data. With the goal of guiding the best care for patients with failing kidney transplants, we summarise the management strategies used during the frequently precarious transition from transplant to dialysis in this review.
Relisting and Repeat Transplant
Over the past 2 decades, transplantation after a failed allograft has increased slowly in absolute terms and actually decreased overall in relative terms (Figure 1), which is somewhat surprising given the rising number of total transplants and the modest gains in long-term allograft outcomes.
![]()
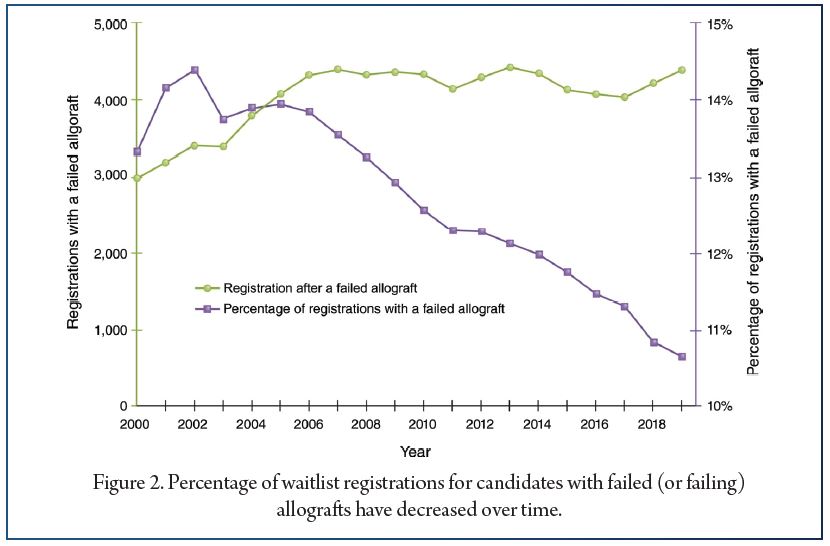
Perhaps more concerning is the fact that, although the total number of candidates being added to the waitlist has increased steadily, the number of candidates with a prior transplant has not kept up; instead, the absolute number of such candidates has remained relatively flat since 2007, resulting in a sharp decline as a proportion of the total number of candidates added to the waitlist (Figure 2).
Immunosuppression Management
Immunoosuppression is one of the most important and complicated aspects in caring for patients with failing and failed allografts. It can affect the probability of repeat transplant, protecting residual kidney function, and preventing the development of graft-intolerance syndrome. Some individuals may benefit from late conversion to belatacept-based regimens, which may allow for an improvement in kidney function and retard rate of decline. It has also been argued that continued immunosuppression in the failed allograft may preserve residual kidney function. However, a few early studies evaluated residual function in a small number of patients with failed allografts initiating peritoneal dialysis and demonstrated a much more rapid decline in function compared with patients with kidney failure without transplant, typically occurring over 6–12 months.
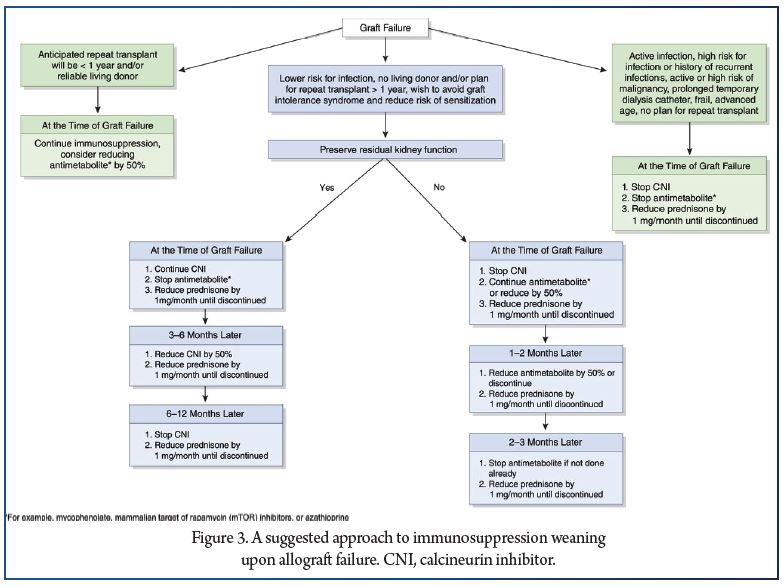
Ultimately, the chance that immunosuppression can preserve some residual kidney function likely depends on whether the underlying etiology of graft failure was immunologic in nature, one of the most common causes of intermediate and late graft loss. Continuing the calcineurin inhibitor may be the best choice for the small subset of patients in which maintaining function is a priority over the ensuing 6–12 months on dialysis, particularly peritoneal dialysis (Figure 3). For the majority of patients, a more rapid taper is likely warranted because there are no published studies that adequately address whether continuing immunosuppression will affect the time course of kidney function decline, especially when taken in the context of the complications associated with these medications.
T.
Allograft Nephrectomy
The potential benefits of nephrectomy must be weighed against the risks of the procedure. There is evidence that removal of the allograft generates donor-specific antibodies, independent of immunosuppression withdrawal. In a recent systematic review of 12 studies, levels of panel reactive antibody ranged from 10% to 55% in patients without allograft nephrectomy, compared with 20%–72% in patients who underwent the procedure. A few hypotheses have been proposed to explain this phenomenon beyond a notably higher risk of blood transfusions. For one, the kidney may behave like a “sponge” that attracts and absorbs formed donor-specific antibodies to their antigenic targets, preventing detection in the serum until the graft is removed. Alternatively, surgery may engender an inflammatory response that promotes antibody formation in the setting of mechanical manipulation, remnant allograft tissue, and increased exposure of antigens.
CKD Management and Dialysis
Modality
The initiation of dialysis is often determined by patient symptoms, but estimates of glomerular filtration and rates of decline may provide additional information. There are several limitations in estimating GFR as a marker of CKD stage in the kidney allograft. Analyses evaluating cystatin C–based equations were previously hindered by lack of a standardized assay. This is particularly troubling given evidence that early referral for patients with native kidney disease is associated with significantly improved clinical care at the start of of dialysis and improved longer-term outcomes a trend that does not appear to extend to transplant nephrologists and their patients with failing allografts. Multidisciplinary clinics dedicated to patients with low-functioning kidney allografts may improve KRT planning, and even reduce emergency-department visits and hospital admissions, although more research is needed. In the absence of such clinics and clear guidelines to assist the nontransplant nephrologist, transplant providers should take some responsibility for patients during this time period.
There should be clear coordination of care among the transplant center and nontransplant nephrologist, with the former focusing on allograft prognosis, immunosuppression weaning, and relisting, and the latter ensuring optimal CKD management and guiding the patient through dialysis planning. Transplant centers may improve this communication by ensuring that patients have a final transplant clinic visit around the time of graft failure, with a standardized, templated note serving as a checklist to make recommendations regarding these issues and establishing continued lines of communications, should the need for shared decision making arise. The optimal timing of dialysis initiation in patients who have received a transplant has been evaluated by several observational studies, but conclusions are limited due to inherent biases and the lack of a specific threshold of function, with similar measures used in native kidney disease to guide care; however, some have raised concerns that early initiation of dialysis could have detrimental consequences on patient outcomes.
Future Directions
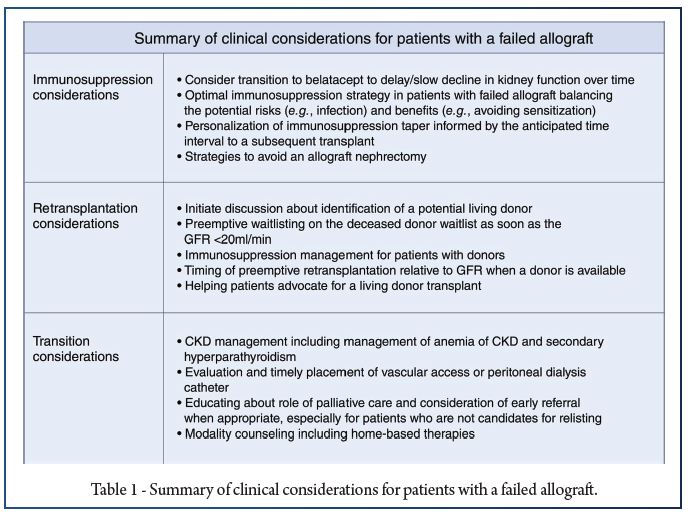
Critical questions about the ideal strategy for managing patients with failing allografts persist on several fronts (Figure 4). We urgently need more data to address the gaps in our clinical understanding of how to manage patients with failing allografts (Table 1).
Conclusion
Many patients undergoing transplant ultimately experience loss of their allograft, and improving intermediate and long-term graft survival continues to be a paramount goal for the transplant community. Until this goal is achieved, it is critical that the care of patients with kidney failure acknowledge and optimize the transition to dialysis and, potentially, back to transplant. In the current environment, patients with a failing allograft often receive suboptimal chronic disease management and dialysis planning and poor continuity of care, and important decisions, with high stakes, are guided by low-quality data. The lack of robust data on optimal clinical management of these patients has contributed to significant variations in clinical practice patterns, with suboptimal outcomes being commonplace for patients. Going forward, if we are to avoid failing our patients, it will be important for the transplant community to recognize these challenges and allocate resources to support the focused, higher-quality research that is required to improve long-term graft survival.
References:
1. Heidari B. Rheumatoid arthritis: early diagnosis and treatment outcomes. Caspian J Intern Med. 2011;2(1):161–70.
2. Miedany YE, Youssef S, Mehanna A, Gaafary ME. Development of a scoring system for assessment of outcome of early undifferentiated inflammatory synovitis. Joint Bone Spine. 2008;75(2):155–62.
3. Birch J, Bhattacharya S. Emerging trends in diagnosis and treatment of rheumatoid arthritis. Prim Care. 2010;37(4):779–92.
4. Nikiphorou E, de Lusignan S, Mallen CD, Khavandi K, Bedarida G, Buckley CD, et al. Cardiovascular risk factors and outcomes in early rheumatoid arthritis: a population-based study. Heart. 2020;106(20):1566–72.
5. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2010;69(9):1580–8.
6. Durand C, Eldoma M, Marshall DA, Bansback N, Hazlewood GS. Patient preferences for disease modifying anti-rheumatic drug treatment in rheumatoid arthritis: a systematic review. J Rheumatol. 2019. https://doi.org/10.3899/jrheum.181165.
7. Gerlag D, Raza K, Lv B, al e. EULAR recommendations for terminology and research in individuals at risk of rheumatoid arthritis: report from the Study Group for Risk Factors for Rheumatoid Arthritis. Ann Rheum Dis. 2012;71(5):638–41.
8. Mankia K, Siddle H, Di Matteo A, Alpízar-Rodríguez D, Kerry J, Kerschbaumer A, et al. A core set of risk factors in individuals at risk of rheumatoid arthritis: a systematic literature review informing the EULAR points to consider for conducting clinical trials and observational studies in individuals at risk of rheumatoid arthritis. RMD Open. 2021;7(3):e001768.
9. Mankia K, Siddle HJ, Kerschbaumer A, Alpizar Rodriguez D, Catrina AI, Cañete JD, et al. EULAR points to consider for conducting clinical trials and observational studies in individuals at risk of rheumatoid arthritis. Ann Rheum Dis. 2021;80(10):1286–98.
10. Niemantsverdriet E, Dakkak YJ, Burgers LE, Bonte-Mineur F, Steup-Beekman GM, van der Kooij SM, et al. TREAT early arthralgia to reverse or limit impending exacerbation to rheumatoid arthritis (TREAT EARLIER): a randomized, double-blind, placebo-controlled clinical trial protocol. Trials. 2020;21(1):862.
11. van Boheemen L, ter Wee M, Turk S, van Beers M, Bos W, Marsman D, et al. The STAtins to Prevent Rheumatoid Arthritis (STAPRA) Trial: clinical results and subsequent qualitative study, a mixed method evaluation. Arthritis Rheum. 2020;72.
12. Gerlag D, Safy M, Maijer K, et al. Effects of B-cell directed therapy on the preclinical stage of rheumatoid arthritis: the PRAIRI study. Ann Rheum Dis. 2019;78(2):179–85.


