
Abstract
The paradigm shift from interferon-based to direct-acting antiviral (DAA) therapy for the treatment of hepatitis C virus (HCV) infection has revolutionized the field of liver transplantation. The advances in effective HCV treatment, along with the persistent shortage in available liver gras, have encouraged investigators to assess the need for adopting more inclusive donor policies. Owing to the poor outcomes following liver transplantation with recurrent HCV infection, liver transplantation using HCV seropositive donors (non-viremic and viremic) had been restricted.
However, as a result of the growing supply of HCV seropositive donors from the recent opioid epidemic along with the advent of ecacious DAA therapy to treat HCV recurrence, there has been an increasing trend to use HCV seropositive donors for both HCV seropositive and seronegative recipients. The review aims to discuss recent advances and associated outcomes related to the use of HCV seropositive grafts for liver transplantation.
Current trends in the demand for liver grafts
Over the past two decades, additional exception policies to the MELD score have been used to further prioritize medical urgency despite geographic location as well as appropriately selecting and transplanting patients with hepatocellular carcinoma. This has led to a signicant rise in the rate of LT surgeries performed, with a landmark 7841 LT surgeries in 2016, the majority of which were from deceased donors.
Moreover, deceased donor LT outcomes have improved; the incidence of post-transplant mortality and graft failure at 1 year decreased to under 10% for recipients. The use of HCV seropositive liver gras has increased because of the availability of eective therapies to treat HCV (DAA agents).
Prior to the availability of DAA agents and during the interferon era, HCV seropositive donors were three times more likely to be discarded than HCV seronegative donors or not considered for procurement at all. Currently, the overall proportion of livers discarded decreased from over 20% in 2010 to 9.0% in 2016; this was likely a reection of the dramatic decrease in discard rates of HCV seropositive non-viremic donors (Fig 1).
Fig 1. Liver Discard Rates
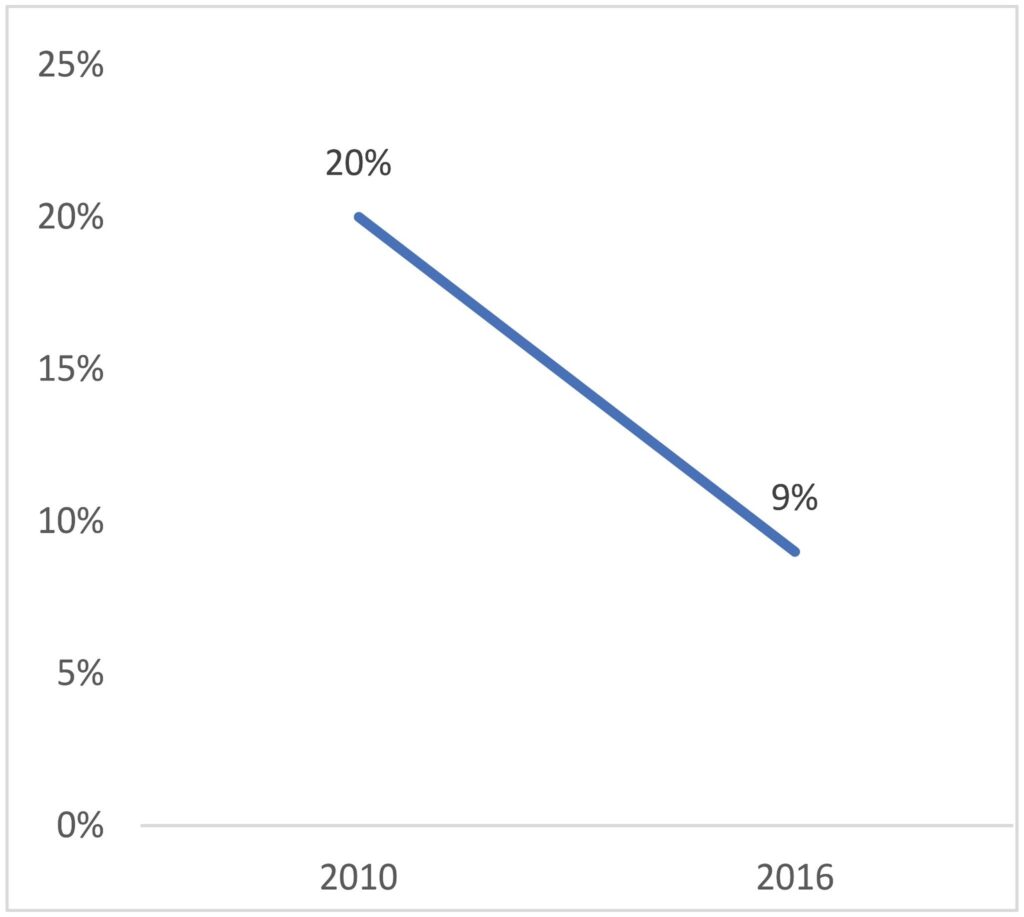
The dramatic reduction in discard rates can be explained in part by the mandated testing for HCV RNA and the ability to identify non-viremic donors.
Natural progression of HCV in the post-transplant setting
A recent analysis has shown cost-effectiveness in treating HCV patients prior to transplantation if the risk of hepatic complications is modiable. The decision for HCV treatment prior to LT depends on the local and regional availability of HCV-positive donors.If there is a high proportion of HCV-positive donors, it may be beneficial to treat after transplantation.
Until 2011, HCV was treated with a combination of pegylated interferon and ribavirin. However, their poor tolerance led to dose reductions or treatment discontinuations. Therefore, interferon therapy was used primarily for treatment of HCV in liver recipients aer transplant only if brosis was seen on biopsy. However, with the advent of DAA agents, treatment of HCV recurrence in early post-transplant has led to improved patient outcomes.
Treatment strategy in HCV recurrence post-transplantation
In 2016, AASLD published treatment guidelines for the recurrence of HCV infection aer transplantation. Patients with chronic HCV received 12 weeks of sofosbuvir/velpatasvir aer recurrence of HCV after transplantation and showed 96% cure. In patients with HCV genotype 2 or 3 infection, non-ribavirin-based formulations include a 12-week daily course of glecaprevir/pibrentasvir or sofosbuvir/velpatasvir for LT recipients with or without compensated cirrhosis.
Particularly, sofosbuvir-based regimens are effective in those with stage IV or V chronic kidney disease. The combination of elbasvir and grazoprevir has been recommended for genotypes 1 and 4 for 12 weeks, and glecaprevir and pibrentasvir for all genotypes for 8 to 16 weeks.
Outcomes of HCV non-viremic and viremic liver donors in HCV-positive recipients
A cohort study among five different US transplant centers from 2002 through 2007 showed that transplantation with HCV seropositive gras was associated with a 58% increased risk of advanced fibrosis. It was also evident that there is a higher prevalence of fibrosis in the group of HCV viremic donors than HCV non-viremic donors. Owing to the risk of advanced brosis, most studies recommend wary use of HCV RNA-positive donors in HCV seropositive patients.
Outcomes of HCV non-viremic and viremic liver grafts into HCV seronegative recipients
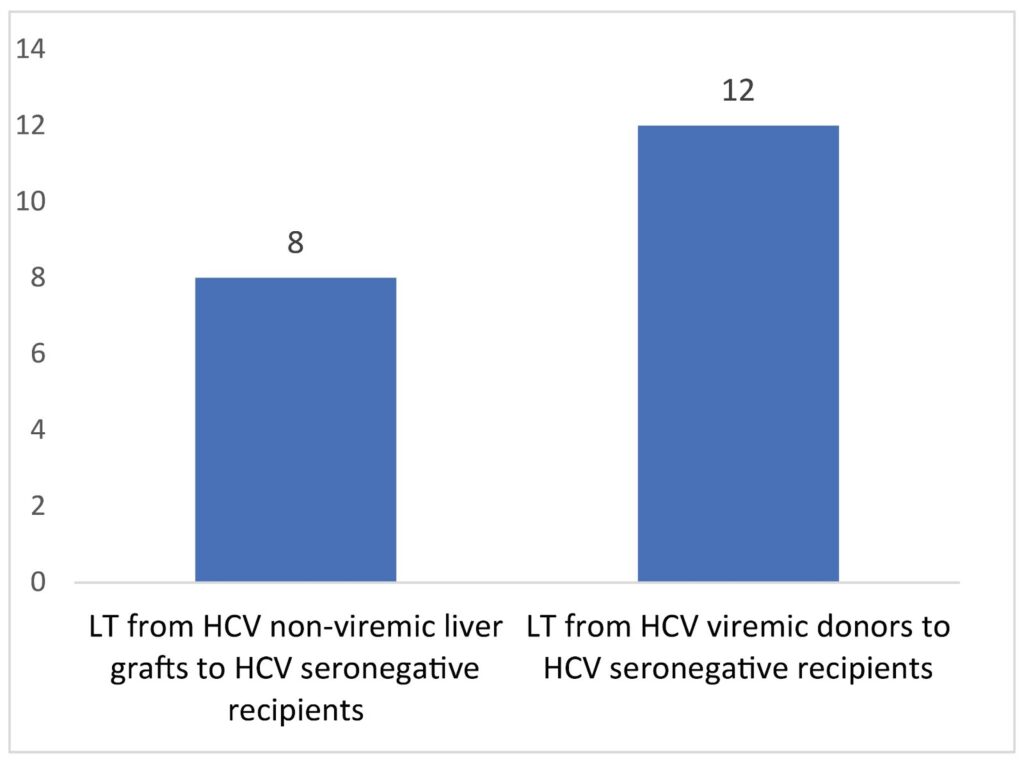
Data regarding the use of HCV seropositive donors in HCV seronegative recipients are limited. Recent studies have evaluated national trends on the use of HCV seropositive donors into HCV seronegative recipients. Since 2017, there was an increase in LT from HCV non-viremic liver gras to HCV seronegative recipients ranging from 1 to 8 per month and LT from HCV viremic donors to HCV seronegative recipients from 1 to 12 per month (Fig 2).
Fig 2. Liver transplant (LT) from HCV non-viremic liver grafts to HCV seronegative recipients
Transplantation of HCV viremic livers into HCV seronegative patients with prophylactic DAA agents could improve patient survival, and benefits may outweigh the harm of introducing a viral infection. Few trials have studied the efficacy of DAA agents for LT from HCV viremic donors to unexposed recipients, and most trials have been conducted in non-LTs.
In a single-center non-randomized trial, non-HCV-infected recipients were treated prophylactically with grazoprevir and elbasvir immediately before and after transplantation from HCV viremic donors, and no HCV RNA was detected in recipients 12 weeks aer prophylactic treatment before or after renal transplantation.
Conclusions
The recent opioid epidemic has resulted in a rising number of deaths among young, otherwise-healthy adults with HCV infection, contributing to the surge in available and used HCV viremic donors with favorable donor criteria. In addition, the era of DAA agents has seen a surge in the use of HCV-infected non-viremic and viremic donors in HCV-unexposed patients with early favorable outcomes in liver, kidney, and heart transplants studied thus far.
References:
- Kim WR, Lake JR, Smith JM, et al. : OPTN/SRTR 2016 Annual Data Report: Liver. Am J Transplant. 2018;18 Suppl 1:172–253. 10.1111/ajt.14559
- Bowring MG, Kucirka LM, Massie AB, et al. : Changes in Utilization and Discard of Hepatitis C-Infected Donor Livers in the Recent Era. Am J Transplant. 2017;17(2):519–27. 10.1111/ajt.13976
- Northup PG, Argo CK, Nguyen DT, et al. : Liver allogras from hepatitis C positive donors can oer good outcomes in hepatitis C positive recipients: A US National Transplant Registry analysis. Transpl Int. 2010;23(10):1038–44. 10.1111/j.1432-2277.2010.01092.x
- Kwo PY, Mantry PS, Coakley E, et al. : An Interferon-free Antiviral Regimen for HCV aer Liver Transplantation. N Engl J Med. 2014;371(25):2375–82. 10.1056/NEJMoa1408921
- Cholankeril G, Ahmed A: Alcoholic Liver Disease Replaces Hepatitis C Virus Infection as the Leading Indication for Liver Transplantation in the United States. Clin Gastroenterol Hepatol. 2018;16(8):1356–8. 10.1016/j.cgh.2017.11.045
- Cholankeril G, Li AA, March KL, et al. : Improved Outcomes in HCV Patients Following Liver Transplantation During the Era of Direct-Acting Antiviral Agents. Clin Gastroenterol Hepatol. 2018;16(3):452–3. 10.1016/j.cgh.2017.08.020
- Gonzalez SA, Troer JF: e rise of the opioid epidemic and hepatitis C-positive organs: A new era in liver transplantation. Hepatology. 2018;67(4):1600–8.10.1002/hep.29572
- U.S. 2016 Surveillance Data for Viral Hepatitis. (2018, April 16); Retrieved November 21, 2019.
- Coer TG, Paul S, Sandıkçı B, et al. : Increasing Utilization and Excellent Initial Outcomes Following Liver Transplant of Hepatitis C Virus (HCV)-Viremic Donors Into HCV-Negative Recipients: Outcomes Following Liver Transplant of HCV-Viremic Donors. Hepatology. 2019;69(6):2381–95. 10.1002/hep.30540
- Starzl TE: History of Liver and Other Splanchnic Organ Transplantation. In: Doria C. (eds) Contemporary Liver Transplantation. Organ and Tissue Transplantation.Springer, Cham,2017; 1–28. 10.1007/978-3-319-05543-5_1-1
- deLemos AS, Vage PA: Expanding the donor pool in liver transplantation: Extended criteria donors. Clin Liver Dis (Hoboken). 2013;2(4):156–159. 10.1002/- cld.222
- Lai JC, O’Leary JG, Troer JF, et al. : Risk of advanced brosis with gras from hepatitis C antibody-positive donors: multicenter cohort study. Liver Transpl. 2012;18(5):532–8. 10.1002/lt.23396
- Levitsky J, Formica RN, Bloom RD, et al. : e American Society of Transplantation Consensus Conference on the Use of Hepatitis C Viremic Donors in Solid Organ Transplantation. Am J Transplant. 2017;17(11):2790–802. 10.1111/ajt.14381
- Berenguer M: Systematic review of the treatment of established recurrent hepatitis C with pegylated interferon in combination with ribavirin. J Hepatol. 2008;49(2):274–87. 10.1016/j.jhep.2008.05.002
- Lile EC, Berenguer M: e New Era of Hepatitis C: erapy in Liver Transplant Recipients. Clin Liver Dis. 2017;21(2):421–34. 10.1016/j.cld.2016.12.012 [
- La NL: Update on the Management of Hepatitis C Virus Infection in the Seing of Chronic Kidney Disease and Kidney Transplantation. Gastroenterol Hepatol (N Y). 2018;14(12):687–705.
- Gadiparthi C, Cholankeril G, Perumpail BJ, et al. : Use of direct-acting antiviral agents in hepatitis C virus-infected liver transplant candidates. World J Gastroenter
- 2018;24(3):315–22. 10.3748/wjg.v24.i3.315
- Cortesi PA, Belli LS, Facchei R, et al. : e optimal timing of hepatitis C therapy in liver transplant-eligible patients: Cost-eectiveness analysis of new opportuni ties. J Viral Hepat. 2018;25(7):791–801. 10.1111/jvh.12877
- Burton MJ: In DAA We Trust: Key Factors Essential to HCV Elimination. Dig Dis Sci. 2019;64(10):2701–2. 10.1007/s10620-019-05748-7
- Jacobson IM, Lawitz E, Gane EJ, et al. : Ecacy of 8 Weeks of Sofosbuvir, Velpatasvir, and Voxilaprevir in Patients With Chronic HCV Infection: 2 Phase 3 Randomized Trials. Gastroenterology. 2017;153(1):113–22. 10.1053/j.gastro.2017.03.047
- Campos-Varela I, Agudelo EZ, Sarkar M, et al. : Use of a hepatitis C virus (HCV) RNA-positive donor in a treated HCV RNA-negative liver transplant recipient. Transpl Infect Dis. 2018;20(1):e12809. 10.1111/tid.12809
- Agarwal K, Castells L, Müllhaupt B, et al. : Sofosbuvir/velpatasvir for 12-weeks in genotype 1-4 HCV-infected liver transplant recipients. Journal of Hepatology. 2018;69(3):603–7. 10.1016/j.jhep.2018.05.039
- Reau N, Kwo PY, Rhee S, et al. : Glecaprevir/Pibrentasvir Treatment in Liver or Kidney Transplant Patients With Hepatitis C Virus Infection. Hepatology. 2018;68(4):1298–307. 10.1002/hep.30046
- Charlton M, Everson GT, Flamm SL, et al. : Ledipasvir and Sofosbuvir Plus Ribavirin for Treatment of HCV Infection in Patients With Advanced Liver Disease. Gastroenterology. 2015;149(3):649–59. 10.1053/j.gastro.2015.05.010
- Feld JJ, Jacobson IM, Hézode C, et al. : Sofosbuvir and Velpatasvir for HCV Genotype 1, 2, 4, 5, and 6 Infection. N Engl J Med. 2015;373(27):2599–607. 10.1056/NEJMoa1512610
- Kwo P, Fried MW, Reddy KR, et al. : Daclatasvir and sofosbuvir treatment of decompensated liver disease or post-liver transplant hepatitis C virus recurrence in patients with advanced liver disease/cirrhosis in a real-world cohort. Hepatol Commun. 2018;2(4):354–63. 10.1002/hep4.1156
- HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C.2018; Retrieved November 21, 2019. Reference Source
- Vargas HE, Laskus T, Wang LF, et al. : Outcome of liver transplantation in hepatitis C virus-infected patients who received hepatitis C virus-infected gras. Gastroenterology. 1999;117(1):149–53. 10.1016/s0016-5085(99)70561-5


