
Introduction
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease characterized by synovial inflammation, bone erosion, and cartilage destruction that leads to joint damage and deformity. Recent advances in pathogenesis and the development of new therapeutic agents and strategies for management have improved clinical outcomes. The most commonly used indices to evaluate disease activity in RA are Disease Activity Score 28 joints (DAS28) and the simplified disease activity index (SDAI). Complete blood count is a simple, inexpensive, and relatively sensitive clinical index that reflects inflammatory response. Neutrophils, lymphocytes, and platelets are potent effector cells in the inflammatory response, and changes in counts of these blood cells in the peripheral blood response to inflammation can be observed in anemia, leukocytosis, and thrombocytopenia. Clinical studies have shown that hematological indices such as neutrophil-to-lymphocyte ratio (NLR) or platelet- to-lysymphocyte ratio (PLR) were higher in patients with RA compared with controls and adequately reflected disease activity status. Recently, the systemic immune-inflammation index (SII) was associated with disease activity in diverse inflammatory rheumatic diseases such as adult-onset Still’s disease (AOSD) and ankylosing spondylitis (AS). However, it has not been evaluated in the correlation of SII and NHL score with traditional disease activity measures in RA. This study aims to determine if different four hematological index, SII, NHL score, NLR and PLR, can be used to assess disease activity in RA using a complete blood count.
Subjects and Methods
The study population consisted of 257 patients with RA and 71 control subjects. The mean age of RA patients and controls was 60.7 years and 60.4 years, respectively, which was not statistically different (Table 1). All participants were female. The mean disease duration of RA was 11.2 years (SD 8.2 years). The levels and these positivity frequencies of RF and anti-CCP antibody were 99.2 IU/mL (87.9%) and 317.4 U/mL (87.2%), respectively. Individual disease activity parameters of swollen joint count (SJC), tender joint count (TJC), patient global assessment (PGA), physician global assessment (PhGA), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) were assessed at the time of study enrollment. PGA and PhGA were assessed using a 100 mm visual analogue scale (VAS). Composite disease activity indices used in RA such as DAS28-ESR, DAS28-CRP, CDAI (clinical disease activity index), and SDAI (simplified disease activity index) were assessed. We arbitrarily classified four disease activity categories remission, low, moderate, and high into three subgroups based on DAS28-ESR, DAS28-CRP, SDAI, and CDAI to compare hematological indices among three disease activity subgroups, as follows; remission, low, and moderate to high disease. Total and differential white blood cells (neutrophils and lymphocytes), hemoglobin, and platelets were assessed from peripheral venous blood obtained from each participant at the time of enrollment in the study. Hematological indices including SII, NHL score, NLR, and PLR were calculated with neutrophils, lymphocytes, hemoglobin, and platelets as follows: SII = platelet × neutrophil/lymphocyte ratio, NHL score = neutrophil/( hemoglobin × lymphocyte) ratio, NLR = neutrophil/ lymphocyte ratio, and PLR = platelet/lymphocyte ratio. The unit of NHL score was g/dL.
Results
Comparison of Hematological Indices between RA Patients and Controls
RA patients had higher white blood count, platelet count, absolute neutrophil count, and percentage of neutrophils compared with controls (p < 0.001, p = 0.002, p < 0.001, and p < 0.001, respectively) (Table 1).

Conversely, RA patients had lower hemoglobin and lymphocyte percentages than controls (p = 0.012 and p < 0.001, respectively). A difference was not observed in absolute lymphocyte count between RA patients and controls. Regarding hematological indices, RA patients showed significantly higher SII, NHL score, NLR, and PLR than controls (p < 0.001, p < 0.001 p < 0.001, and p = 0.046, respectively). There were significant differences in hematological indices between RA and control groups.
Correlation between Hematological Indices & Disease Activity Parameters
SII was positively associated with ESR, CRP, SJC, PGA, PhGA, DAS28-ESR, DAS28-CRP, CDAI, and SDAI but not with TJC. NHL score was associated with most of all measured activity parameters except for ESR and TJC. NLR was associated with CRP, SJC, PhGA, DAS28-CRP, CDAI, and SDAI. PLR was associated only with CRP but not with other disease parameters. There were no differences in SII, NHL score, NLR, and PLR between RF-positive and -negative patients. The values of all hematological indices were not different according to the presence of anti-CCP antibody. This analysis suggested that hematological indices were generally associated with composite or individual indices of disease activity in patients with RA.
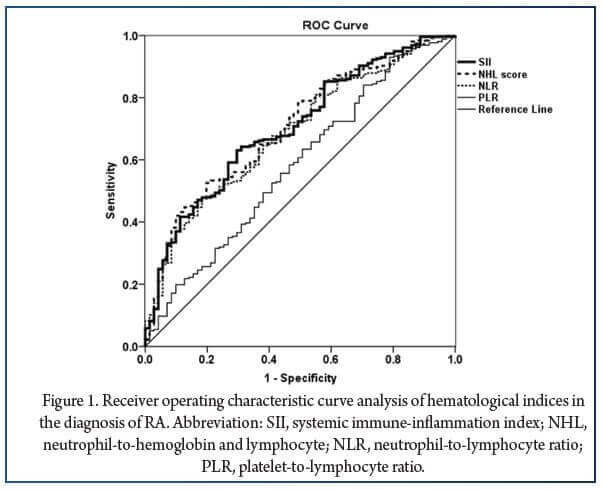
Assessment of Accuracy of Hematological Indices for the Diagnosis and Remission in RA Using ROC Curve
The ROC analysis was used to determine the diagnostic accuracy of hematological indices in RA. In the ROC analysis, RA was used as the state variable, and hematological indices of SII, NHL score, NLR, and PLR were used as the test variables (Figure 1). The AUC for each hematological index was 0.703 (95% CI 0.637–0.769, p < 0.001) for SII, 0.705 (95% CI 0.639–0.770, p < 0.001) for NHL score, 0.686 (95% CI 0.619–0.753, p < 0.001) for NLR, and 0.581 (95% CI 0.505–0.658, p = 0.036) for PLR. The AUC for ESR and CRP was 0.622 (95% CI 0.552–0.693, p = 0.002) and 0.660 (95% CI 0.593–0.727, p < 0.001), respectively. In addition, the ROC analysis showed that the optimal cut-off values for the presence of RA were 305.6 for SII and 0.112 for NHL score, respectively. Moreover, 85% sensitivity and 42% specificity for SII and 78% sensitivity and 49% specificity for NHL score were yielded based on the Youden’s index. The results showed that SII and NHL score might be statistically acceptable indices for the diagnosis of RA rather than other hematologic indices such as NLR and PLR and acute phase reactants including ESR and CRP.
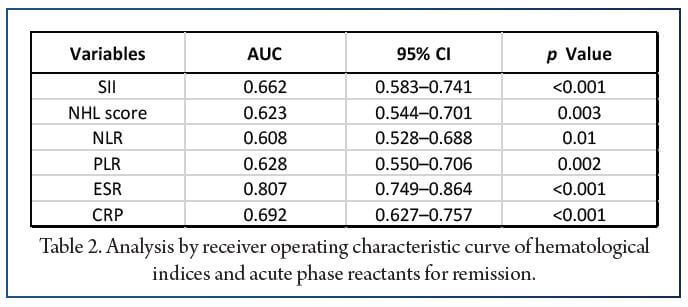
In addition, the evaluation of efficacy for remission was performed using ROC curves. The AUC obtained from all hematological indices ranged from 0.608 to 0.628, indicating that these hematological indices were too weak to determine clinical remission, although they were statistically significant (Table 2). However, ESR showed significant accuracy for remission but not CRP (AUC = 0.807 for ESR and AUC = 0.692 for CRP, respectively).
Conclusions
In conclusion, hematological indices are easily measured and available disease activity markers of systemic inflammation in RA. Among hematological indices, SII, NHL score, & NLR, but not PLR, were associated with disease activity measures & adequately reflected disease activity in RA. Furthermore, two indices, SII and NHL score, could have a complementary role in the diagnosis of RA. Thus, these hematological indices, along with the traditional measures, are helpful in assessing the disease activity of RA in clinical practice. The role of hematological indices in the assessment of disease activity and prediction of clinical outcome should be confirmed in prospective longitudinal studies.
References:
1. Aletaha, D.; Smolen, J.S. Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef].
2. Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Res. 2018, 6, 15.
3. Anderson, J.K.; Zimmerman, L.; Caplan, L.; Michaud, K. Measures of rheumatoid arthritis disease activity: Patient (PtGA) and Provider (PrGA) Global Assessment of Disease Activity, Disease Activity Score (DAS) and Disease Activity Score with 28-Joint Counts (DAS28), Simplified Disease Activity Index (SDAI), Clinical Disease Activity Index (CDAI), Patient Activity Score (PAS) and Patient Activity Score-II (PASII), Routine Assessment of Patient Index Data (RAPID), Rheumatoid Arthritis Disease Activity Index (RADAI) and Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5), Chronic Arthritis Systemic Index (CASI), Patient-Based Disease Activity Score With ESR (PDAS1) and Patient-Based Disease Activity Score without ESR (PDAS2), and Mean Overall Index for Rheumatoid Arthritis (MOI-RA). Arthritis Care. Res. 2011, 63 (Suppl. 11), S14–S36.
4. van der Heijde, D.M.; van ‘t Hof, M.; van Riel, P.L.; van de Putte, L.B. Development of a disease activity score based on judgment in clinical practice by rheumatologists. J. Rheumatol. 1993, 20, 579–581.
5. Smolen, J.S.; Breedveld, F.C.; Schiff, M.H.; Kalden, J.R.; Emery, P.; Eberl, G.; van Riel, P.L.; Tugwell, P. A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology 2003, 42, 244–257.
6. Aletaha, D.; Smolen, J. The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): A review of their usefulness and validity in rheumatoid arthritis. Clin. Exp. Rheumatol. 2005, 23, S100–S108.
7. Boilard, E.; Nigrovic, P.A.; Larabee, K.; Watts, G.F.; Coblyn, J.S.; Weinblatt, M.E.; Massarotti, E.M.; Remold-O’Donnell, E.; Farndale, R.W.; Ware, J.; et al. Platelets amplify inflammation in arthritis via collagen-dependent microparticle production. Science 2010, 327, 580–583.
8. Scapini, P.; Cassatella, M.A. Social networking of human neutrophils within the immune system. Blood 2014, 124, 710–719.
9. Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454.
10. Maden, M.; Pamuk, G.E.; Pamuk, Ö.N. Development of Atherosclerotic Cardiovascular Mortality in Gouty Arthritis and Rheumatoid Arthritis Patients: Are They Associated With Mean Platelet Volume and Neutrophil-Lymphocyte Ratio? A Comparative Study. Arch. Rheumatol. 2017, 32, 39–45.
11. Uslu, A.U.; Küçük, A.; Sahin, A.; Ugan, Y.; Yılmaz, R.; Güngör, T.; Bagcacı, S.; Küçüksen, S. Two new inflammatory markers associated with Disease Activity Score-28 in patients with rheumatoid arthritis: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Int. J. Rheum. Dis. 2015, 18, 731–735.
12. Sargin, G.; Senturk, T.; Yavasoglu, I.; Kose, R. Relationship between neutrophil-lymphocyte, platelet-lymphocyte ratio and disease activity in rheumatoid arthritis treated with rituximab. Int. J. Rheum. Dis. 2018, 21, 2122–2127.
13. Tekeoglu, I.; Gürol, G.; Harman, H.; Karakeçe, E.; Çiftci, I.H. Overlooked hematological markers of disease activity in rheumatoid arthritis. Int. J. Rheum. Dis. 2016, 19, 1078–1082.
14. Yolbas, S.; Yildirim, A.; Gozel, N.; Uz, B.; Koca, S.S. Hematological Indices May Be Useful in the Diagnosis of Systemic Lupus Erythematosus and in Determining Disease Activity in Behçet’s Disease. Med. Princ. Pract. 2016, 25, 510–516.
15. Mercan, R.; Bitik, B.; Tufan, A.; Bozbulut, U.B.; Atas, N.; Ozturk, M.A.; Haznedaroglu, S.; Goker, B. The Association Between Neutrophil/Lymphocyte Ratio and Disease Activity in Rheumatoid Arthritis and Ankylosing Spondylitis. J. Clin. Lab. Anal. 2016, 30, 597–601.
16. Fu, H.; Qin, B.; Hu, Z.; Ma, N.; Yang, M.; Wei, T.; Tang, Q.; Huang, Y.; Huang, F.; Liang, Y.; et al. Neutrophil- and platelet-to-lymphocyte ratios are correlated with disease activity in rheumatoid arthritis. Clin. Lab. 2015, 61, 269–273.
17. Lee, H.N.; Kim, Y.K.; Kim, G.T.; Ahn, E.; So, M.W.; Sohn, D.H.; Lee, S.G. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio as predictors of 12-week treatment response and drug persistence of anti-tumor necrosis factor- agents in patients with rheumatoid arthritis: A retrospective chart review analysis. Rheumatol. Int. 2019, 39, 859–868.
18. Kim, J.W.; Jung, J.Y.; Suh, C.H.; Kim, H.A. Systemic immune-inflammation index combined with ferritin can serve as a reliable assessment score for adult-onset Still’s disease. Clin. Rheumatol. 2021, 40, 661–668.
19. Kim, Y.; Choi, H.; Jung, S.M.; Song, J.J.; Park, Y.B.; Lee, S.W. Systemic immune-inflammation index could estimate the cross-sectional high activity and the poor outcomes in immunosuppressive drug-naïve patients with antineutrophil cytoplasmic antibody-associated vasculitis. Nephrology 2019, 24, 711–717.
20. Wu, J.; Yan, L.; Chai, K. Systemic immune-inflammation index is associated with disease activity in patients with ankylosing spondylitis. J. Clin. Lab. Anal. 2021, 35, e23964.
21. Kim, H.J.; Lee, J.H.; Jang, S.Y.; Bae, M.H.; Yang, D.H.; Park, H.S.; Cho, Y.K.; Jeong, M.H.; Park, J.S.; Kim, H.S.; et al. Prognostic value of novel neutrophil-to-hemoglobin and lymphocyte score in patients with acute myocardial infarction. Eur. J. Inflamm. 2021, 19, 20587392211039095.
22. Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis. Rheum. 2010, 62, 2569–2581.


