
Introduction
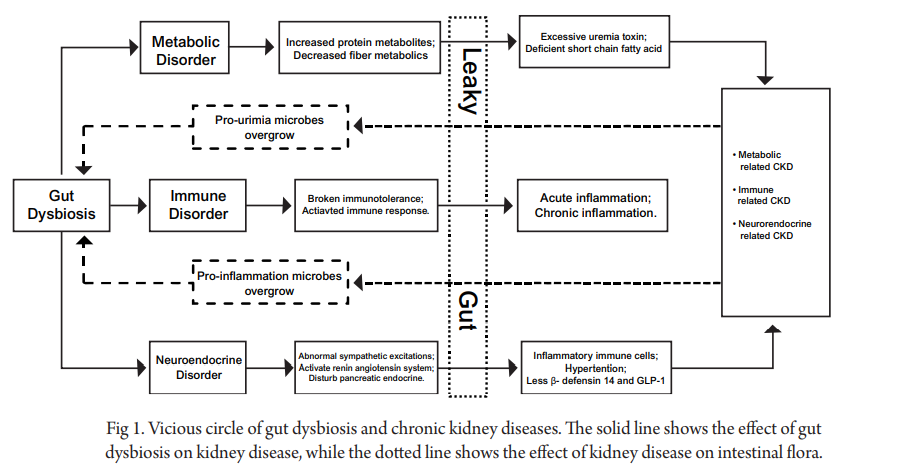
Gut dysbiosis may be involved in the pathophysiology of CKD and the relationship between the intestine and kidney is referred to as the ‘gut-kidney axis,’ in which the gut microbiota is an essential component. Gut dysbiosis is a condition in which the microbiota is abnormally abundant which can lead to immunological, metabolic, or endocrine issues. It may cause an imbalance in immunological responses and tolerance which may contribute to the initiation and progression of CKD.
Metabolites derived from gut microbiota, such as trimethylamine-N-oxide (TMAO), p-cresyl sulphate (PCS), indoxyl sulphate (IS), and phenylacetylglutamine (PAG), as well as fermentation products may contribute to declining kidney function and worsening cardiovascular diseases, whereas short-chain fatty acids (SCFAs), fermentation products of dietary fibre exert protective effects on the kidney (Fig 1.) This study performed a systematic review to analyze the bacterial diversity in patients with CKD.
Study Protocol
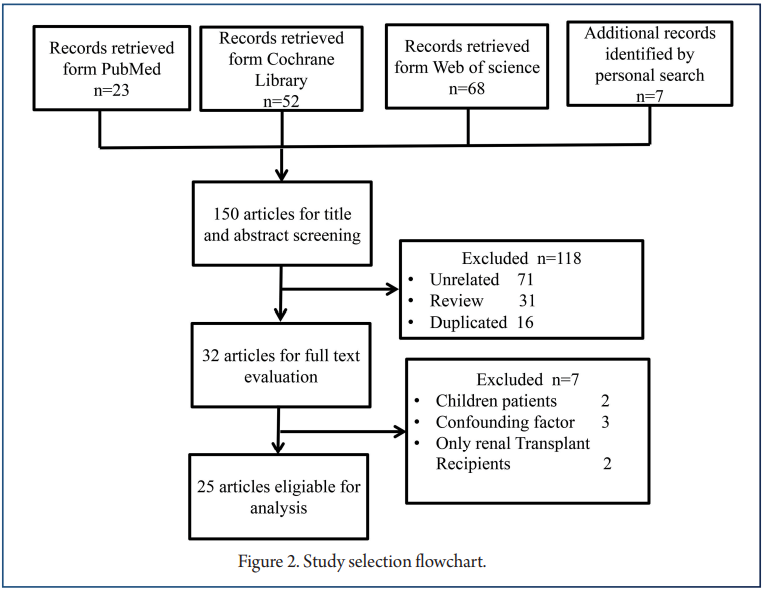
A total of 150 records were retrieved; 25, ranging from 2012 to 2020, were eligible for inclusion in our systematic review (Figure 2).
The 25 studies included 1436 patients with CKD and 918 healthy controls. Nine studies focused on ESRD; 12 focused on CKD ranging in severity from stage 1 to 5; and four focused on two specific pathological types of CKD: IgA nephropathy (IgAN) and DN. Seventeen studies were carried out in China, three in the US, two in Italy, and one in Austria, Brazil, and Netherlands.
Nineteen studies conducted full-scale analysis of the gut microbial profile, while six were limited to specific bacteria at the species level and mainly applied polymerase chain reaction (PCR) analysis. Patients in eight studies received renal replacement therapy including hemodialysis (n = 419), peritoneal dialysis (n = 68), or kidney transplantation (n = 20).
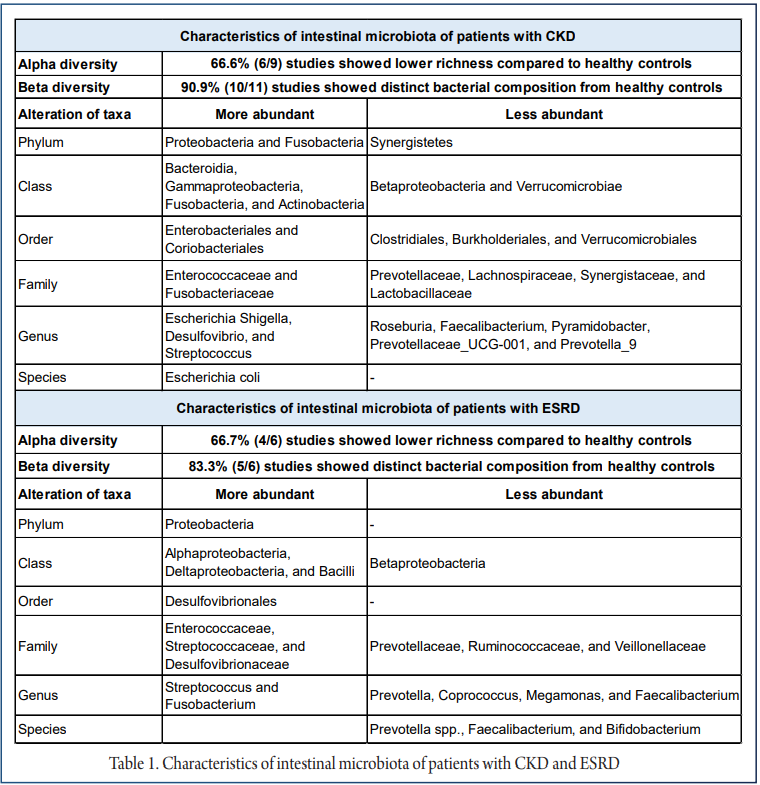
The study summarized the existing evidence describing the profile of gut microbiota in patients with CKD or ESRD with the aim of identifying specific microbial taxa that could contribute to disease pathogenesis. The progression could form the basis for new approaches to modulate gut dysbiosis to treat and prevent CKD. The alterations in gut microbial profiles in patients with CKD or ESRD were determined and are shown in Table 1.
Conclusion
The current study supports the increased abundance of phylum Proteobacteria and Fusobacteria, genus Escherichia Shigella, Desulfovibrio, and Streptococcus, while lower abundance of genus Roseburia, Faecalibacterium, Pyramidobacter, Prevotellaceae UCG-001, and Prevotella 9 in patients with CKD; and increased abundance of phylum Proteobacteria, and genus Streptococcus and Fusobacterium, while lower abundance of Prevotella, Coprococcus, Megamonas, and Faecalibacterium in patients with ESRD.
Furthermore, advanced CKD patients had greater TMAO and PCS concentrations but lower SCFA concentrations. However, due to the variability of the available data, the features of the gut microbiota in individuals with CKD were not established. Further research should use high-throughput sequencing technology and comprehensive reporting to gain a better understanding of the gut microbiota, which could lead to a better understanding of the underlying mechanisms of how the gut microbiota interacts with CKD and its potential implications in CKD treatment and prevention.
References
1. Saran R, Robinson B, Abbott KC, et al. US Renal Data System 2017 Annual Data Report: epidemiology of kidney disease in the United States. Am J Kidney Dis. 2018;71(3):A7.
2. Zhang L, Wang F, Wang L, et al. Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet (London, England). 2012;379(9818):815–822.
3. Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038–2047.
4. Hallan SI, Coresh J, Astor BC, et al. International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol. 2006;17(8):2275–2284.
5. Yang T, Richards EM, Pepine CJ, et al. The gut microbiota and the brain-gut-kidney axis in hypertension and chronic kidney disease. Nat Rev Nephrol. 2018;14(7):442–456.
6. Meijers B, Evenepoel P, Anders HJ. Intestinal microbiome and fitness in kidney disease. Nat Rev Nephrol. 2019;15(9):531–545.
7. Evenepoel P, Poesen R, Meijers B. The gut-kidney axis. Pediatr Nephrol. 2017;32(11):2005–2014.
8. Honda K, Littman DR. The microbiota in adaptive immune homeostasis and disease. Nature. 2016;535(7610):75–84.
9. Thaiss CA, Zmora N, Levy M, et al. The microbiome and innate immunity. Nature. 2016;535(7610):65–74.
10. Briskey D, Tucker P, Johnson DW, et al. The role of the gastrointestinal tract and microbiota on uremic toxins and chronic kidney disease development. Clin Exp Nephrol. 2017;21(1):7–15.
11. Wong J, Piceno YM, DeSantis TZ, et al. Expansion of urease- and uricase-containing, indole- and p-cresol-forming and contraction of short-chain fatty acid-producing intestinal microbiota in ESRD. Am J Nephrol. 2014;39(3):230–237.
12. Lu CC, Ma KL, Ruan XZ, et al. Intestinal dysbiosis activates renal renin–angiotensin system contributing to incipient diabetic nephropathy. Int J Med Sci. 2018;15(8):816–822.
13. Everard A, Cani PD. Gut microbiota and GLP-1. Rev Endocr Metab Disord. 2014;15(3):189–196.
14. Vaziri ND, Zhao YY, Pahl MV. Altered intestinal microbial flora and impaired epithelial barrier structure and function in CKD: the nature, mechanisms, consequences and potential treatment. Nephrol Dial Transplant. 2016;31(5):737–746.
15. Wang F, Jiang H, Shi K, et al. Gut bacterial translocation is associated with microinflammation in end-stage renal disease patients. Nephrology (Carlton). 2012;17(8):733–738.
16. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605.
17. Zhong Z, Tan J, Tan L, et al. Modifications of gut microbiota are associated with the severity of IgA nephropathy in the Chinese population. Int Immunopharmacol. 2020;89:107085.
18. Hu X, Du J, Xie Y, et al. Fecal microbiota characteristics of Chinese patients with primary IgA nephropathy: a cross-sectional study. BMC Nephrol. 2020;21(1):97.
19. De Angelis M, Montemurno E, Piccolo M, et al. Microbiota and metabolome associated with immunoglobulin A nephropathy (IgAN). PLoS One. 2014;9(6):e99006.
20. Tao S, Li L, Li L, et al. Understanding the gut-kidney axis among biopsy-proven diabetic nephropathy, type 2 diabetes mellitus and healthy controls: an analysis of the gut microbiota composition. Acta Diabetol. 2019;56(5):581–592.


