
Background
An increasing percentage of potential organ donors are infected with hepatitis C virus (HCV). After transplantation from an infected donor, establishment of HCV infection in uninfected recipients is near-universal, with the requirement for post-transplant antiviral treatment. The aim of this study was to determine if antiviral drugs combined with an HCV entry blocker given before and for 7 days after transplant would be safe and reduce the likelihood of HCV infection in recipients of organs from HCV-infected donors.
Methods
HCV-uninfected organ recipients without pre-existing liver disease were treated with ezetimibe (10 mg; an HCV entry inhibitor) and glecaprevir-pibrentasvir (300 mg/120 mg) before and after transplantation from HCV-infected donors aged younger than 70 years. Recipients received a single dose 6–12 h before transplant and once a day for 7 days after surgery (eight doses in total). HCV RNA was assessed once a day for 14 days and then once a week until 12 weeks post-transplant. The primary endpoint was prevention of chronic HCV infection, as evidenced by undetectable serum HCV RNA at 12 weeks after transplant, and assessed in the intention-to-treat population. 12-week data are reported for the first 30 patients.
Findings
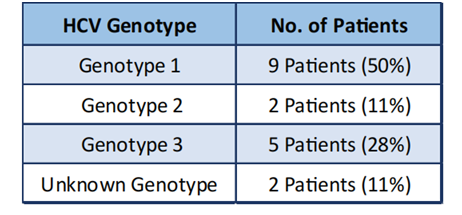
30 patients, 23 men and seven women; median age 61 years received transplants from 18 HCV-infected donors. The median donor viral load was 5·11 log10IU/mL and at least three HCV genotypes were represented, nine [50%] donors with genotype 1, two [11%] with genotype 2, ‑ve [28%] with genotype 3, and two [11%] with unknown genotype.
Table 1. HCV Genotype in transplant patients
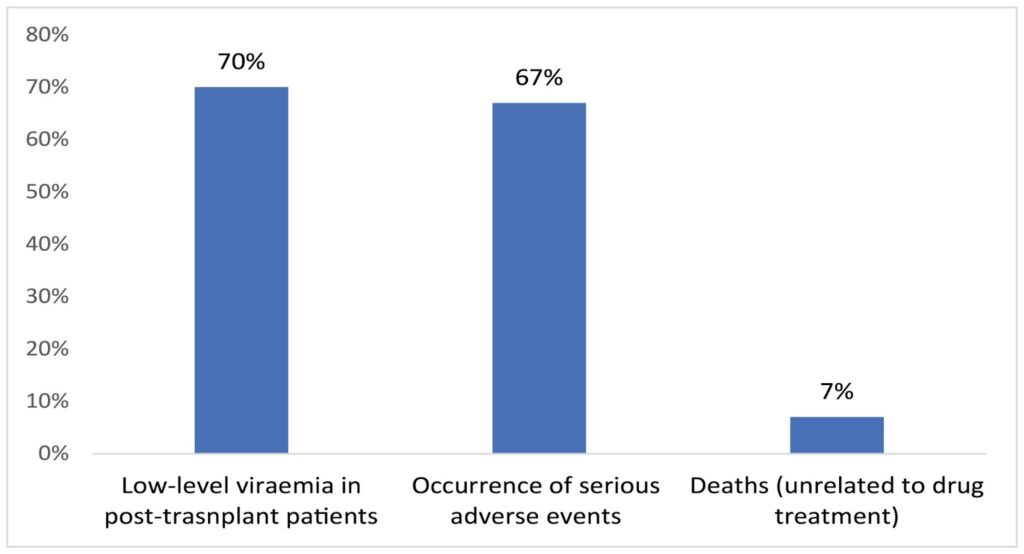
All 30 transplant recipients met the primary endpoint of undetectable HCV RNA at 12 weeks post-transplant, and were HCV RNA-negative at last follow-up. Low-level viraemia was transiently detectable in 21 (70%) of 30 recipients in the early post-transplant period but not after day 14 (Fig 1). 32 serious adverse events occurred in 20 (67%) recipients, with one grade 3 elevations in alanine aminotransferase (ALT) possibly related to treatment. Among the serious adverse events were two recipient deaths due to causes unrelated to study drug treatment with neither patient ever being viraemic for HCV (Fig 1).
Fig 1. Study findings in 30 transplant recipients
Interpretation
Ezetimibe combined with glecaprevir-pibrentasvir given one dose before and for 7 days aer transplant prevented the establishment of chronic HCV infection in recipients of different organs from HCV-infected donors. This study shows that an ultra-short course of direct acting antivirals and ezetimibe can prevent the establishment of chronic HCV infection in the recipient, alleviating many of the concerns with transplanting organs from HCV-infected donors.
References
- Durand CM Bowring MG omas AG et al. e drug overdose epidemic and deceased-donor transplantation in the United States: a national registry study. Ann Intern Med. 2018; 168: 702-711
- Feld JJ Jacobson IM Hézode C et al. Sofosbuvir and velpatasvir for HCV genotype 1, 2, 4, 5, and 6 infection. N Engl J Med. 2015; 373: 2599-2607
- Zeuzem S Foster GR Wang S et al. Glecaprevir–pibrentasvir for 8 or 12 weeks in HCV genotype 1 or 3 infection. N Engl J Med. 2018; 378: 354-369
- Durand CM Bowring MG Brown DM et al. Direct-acting antiviral prophylaxis in kidney transplantation from hepatitis C virus-infected donors to noninfected recipients: an open-label nonrandomized trial. Ann Intern Med. 2018; 168: 533-540
- Woolley AE Singh SK Goldberg HJ et al. Heart and lung transplants from HCV-infected donors to uninfected recipients. N Engl J Med. 2019; 380: 1606-1617
- Goldberg DS Abt PL Blumberg EA et al. Trial of transplantation of HCV-infected kidneys into uninfected recipients. N Engl J Med. 2017; 376: 2394-2395
- Cypel M Feld JJ Galasso M et al. Prevention of viral transmission during lung transplantation with hepatitis C-viraemic donors: an open-label, single-centre, pilot trial. Lancet Respir Med. 2020; 8: 192-201
- Levitsky J Formica RN Bloom RD et al. e American Society of Transplantation consensus conference on the use of hepatitis C viremic donors in solid organ transplantation. Am J Transplant. 2017; 17: 2790-2802
- Kapila N Al-Khallou‑ K Bejarano PA Vanaa JM Zervos XB. Fibrosing cholestatic hepatitis aer kidney transplantation from HCV-viremic donors to HCV-negative recipients: a unique complication in the DAA era. Am J Transplant. 2020; 20: 600-605
- Kapila N Menon KVN Al-Khallou‑ K et al. HCV NAT positive solid organ allogras transplanted into HCV negative recipients: a real-world experience. Hepatolo[1]gy. 2019; (published online Oct 28.) DOI:10.1002/hep.31011
- Galasso M Feld JJ Watanabe Y et al. Inactivating hepatitis C virus in donor lungs using light therapies during normothermic ex vivo lung perfusion. Nat Commun. 2019; 10: 481
- Pileri P Uematsu Y Campagnoli S et al. Binding of hepatitis C virus to CD81. Science. 1998;282: 938-941
- Lavie M Sarrazin S Montserret R et al. Identi‑cation of conserved residues in hepatitis C virus envelope glycoprotein E2 that modulate virus dependence on CD81 and SRB1 entry factors. J Virol. 2014; 88: 10584-10597
- Evans MJ von Hahn T Tscherne DM et al. Claudin-1 is a hepatitis C virus co-receptor required for a late step in entry. Nature. 2007; 446: 801-805
- Ploss A Evans MJ Gaysinskaya VA et al.Human occludin is a hepatitis C virus entry factor required for infection of mouse cells. Nature. 2009; 457: 882-886
- Sainz Jr, B Barreo N Martin DN et al. Identi‑cation of the Niemann-Pick C1-like 1 cholesterol absorption receptor as a new hepatitis C virus entry factor. Nat Med. 2012; 18: 281-285
- Forns X Lee SS Valdes J et al. Glecaprevir plus pibrentasvir for chronic hepatitis C virus genotype 1, 2, 4, 5, or 6 infection in adults with compensated cirrhosis (EXPEDITION-1): a single-arm, open-label, multicentre phase 3 trial. Lancet Infect Dis. 2017; 17: 1062-1068
- Gane E Lawitz E Pugatch D et al. Glecaprevir and pibrentasvir in patients with HCV and severe renal impairment. N Engl J Med. 2017; 377: 1448-1455
- Bedossa P Poynard T An algorithm for grading activity in chronic hepatitis C. Hepatology. 1996; 24: 289-293
- Cypel M Yeung JC Liu M et al. Normothermic ex vivo lung perfusion in clinical lung transplantation. N Engl J Med. 2011; 364: 1431-1440
- Kosloski MP Zhao W Li H et al. Drug-drug interactions of tacrolimus or cyclosporine with glecaprevir and pibrentasvir in healthy subjects. Clin Pharmacol Drug Dev. 2019; 8: 779-789
- Slim H ompson PD Ezetimibe-related myopathy: a systematic review. J Clin Lipidol. 2008; 2: 328-334
- Goldberg DS Levitsky J Transplanting livers from HCV-infected donors into HCV-negative recipients: promise but mind the pitfalls. Am J Transplant. 2019; 19: 1264-1265
- Molnar MZ Nair S Cseprekal O et al. Transplantation of kidneys from hepatitis C-infected donors to hepatitis C-negative recipients: single center experience. Am J Transplant. 2019; 19: 3046-3057
- Komurian-Pradel F Perret M Deiman B et al. Strand speci‑c quantitative real-time PCR to study replication of hepatitis C virus genome. J Virol Methods. 2004; 116: 103-106
- Foster GR Afdhal N Roberts SK et al. Sofosbuvir and velpatasvir for HCV genotype 2 and 3 infection. N Engl J Med. 2015; 373: 2608-2617
- Kohli A Osinusi A Sims Z et al. Virological response aer 6 week triple-drug regimens for hepatitis C: a proof-of-concept phase 2A cohort study. Lancet. 2015; 385: 1107-1113
- de Vera ME Volk ML Ncube Z et al. Transplantation of hepatitis C virus (HCV) antibody positive, nucleic acid test negative donor kidneys to HCV negative patients frequently results in seroconversion but not HCV viremia. Am J Transplant. 2018; 18: 2451-2456
- Reese PP Abt PL Blumberg EA et al. Twelve-month outcomes a er transplant of hepatitis C-infected kidneys into uninfected recipients: a single-group trial. Ann Intern Med. 2018; 169: 273-281
- Fontaine H Lazarus A Pol S et al.Bradyarrhythmias associated with sofosbuvir treatment. N Engl J Med. 2015; 373: 1886-1888
- American Association for the Study of Liver Diseases and Infectious Diseases Society of America HCV Guidance Panel Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology. 2015; 62: 932-954
- Gupta G Yakubu I Bhati C et al. Ultra-short duration direct acting anti-viral prophylaxis to prevent virus transmission from hepatitis C viremic donors to hepatitis c negative kidney transplant recipients. Am J Transplant. 2020; 20: 739-751
- Bethea ED Gaj K Gustafson JL et al. Pre-emptive pangenotypic direct acting antiviral therapy in donor HCV-positive to recipient HCV-negative heart transplantation: an open-label study. Lancet Gastroenterol Hepatol. 2019; 4: 771-780


