
Introduction
In recent years, advancements in understanding allorecognition and graft rejection mechanisms have revealed a complex immune response involving multiple pathways. Current transplant monitoring relies on traditional markers such as serum creatinine, proteinuria, and drug blood levels, along with donor-specific antibodies. However, emerging “omic” technologies have identified novel biomarkers that show promise for improving transplant monitoring. These include urinary chemokines, measurement of cell-free DNA of donor origin, transcriptomics, metabolomics, proteomics, and the study of extracellular vesicles. While these new biomarkers offer potential benefits in early identification of rejection and predictive value, their high costs and limited clinical applicability currently hinder widespread use. Integrating these new biomarkers with traditional tools could enable earlier detection of rejection and prompt therapeutic intervention. This review explores the strengths, limitations, and future applications of traditional and novel biomarkers, both invasive and non-invasive, in the context of pediatric transplantation.
The ideal biomarker
Biomarkers are defined as measurable characteristics that indicate normal or pathological biological processes. They can be used for diagnosis, monitoring, predicting treatment response and prognosis, assessing safety, and identifying susceptibility or risk. Key characteristics of an ideal biomarker include accurate identification of high-risk patients, high diagnostic accuracy, predictive value, and responsiveness to treatment. Biomarkers should also demonstrate reproducibility, interpretability, and external validation. Additionally, biomarkers can serve as surrogate endpoints, allowing for early detection of certain conditions and guiding appropriate interventions. In the field of transplantation, biomarkers could potentially be used as thresholds for biopsy or treatment decisions related to rejection.
Traditional biomarkers in transplantation and their limitations
Creatinine, proteinuria, and drug blood levels are commonly used biomarkers in kidney transplantation. However, they have limitations in terms of specificity, sensitivity, and early detection of rejection. Surveillance protocol biopsies, though invasive, are considered the gold standard for assessing graft health. Donor-specific antibodies (DSA) are important biomarkers associated with poor graft outcomes, and their monitoring is recommended. Non-donor-specific anti-HLA antibodies and non-HLA antibodies are also being studied for their potential role in rejection. The use of additional noninvasive or minimally invasive biomarkers is needed to improve monitoring and personalize therapy in transplant recipients.
Surveillance protocol biopsy
Surveillance protocol biopsy is currently considered the gold standard for assessing the health of a transplanted kidney. However, there are debates about its specificity, sensitivity, and predictive value, especially when performed early after transplantation. These biopsies are invasive and carry risks of adverse events, such as bleeding and artero-venous fistula. They are time-consuming and require pathology interpretation. They are typically limited to the first 12-24 months after transplantation. The role of protocol biopsies in improving long-term graft survival in children is still debated due to various factors such as different immunosuppressive regimens and timing of biopsies. The incidental finding of non-specific signs of chronic allograft damage without actionable inflammation is also a concern. Subclinical signs of rejection are sometimes detected in patients without apparent symptoms. Some studies suggest the benefits of preemptive treatment based on these findings. There is ongoing controversy regarding the necessity of repeated histology monitoring, and controlled studies are needed. The limitations and challenges of surveillance biopsies highlight the need for additional noninvasive or minimally invasive monitoring methods that can be easily and widely implemented to continuously detect subclinical rejection, assess treatment response, and optimize therapy in a personalized manner.
Drug level monitoring
Drug level monitoring is an essential tool for assessing immunosuppressive drug use in transplantation. While single sample trough concentrations are inadequate for drugs like mycophenolic acid, estimating the area under the curve (AUC) provides a more accurate measure of drug exposure. Tacrolimus intra-patient variability (IPV) has been linked to complications such as rejection and graft loss, although its correlation is weaker in pediatric studies. Future perspectives include the development of expert systems for drug exposure estimation, techniques for simultaneous evaluation of multiple drugs, and the adoption of “time in therapeutic range” as a predictor of under-suppression and the risk of allograft rejection.
Donor-specific antibodies
Donor-specific antibodies (DSA) are antibodies produced by transplant recipients against specific HLA antigens on the donor kidney. DSA-mediated rejection can be acute or chronic, with acute rejection occurring rapidly due to high-titer DSA and chronic rejection developing gradually with varying antibody titers. DSA can damage the kidney by affecting the basement membrane or causing arteriopathy. De novo DSA (dnDSA) after transplantation is associated with poor graft outcomes and is considered a biomarker for late acute rejection, chronic rejection, transplant glomerulopathy, and graft loss. Monitoring DSA regularly is important, and the characteristics of the antibody, such as the IgG subclass, can influence its clinical relevance. Higher levels of DSA, measured using Luminex technology, are generally associated with impaired graft function. While therapeutic strategies to reduce DSA levels are being investigated, preventing initial DSA formation and identifying risk factors for DSA development are Different immunosuppressive therapies may impact DSA development, with calcineurin inhibitors potentially being less associated with DSA formation compared to mTOR inhibitors or lower mycophenolic acid levels.
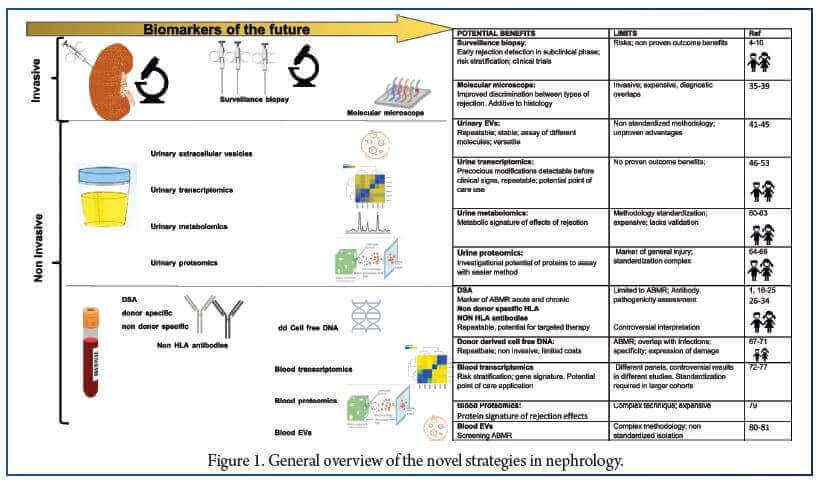
Biomarkers of the future
Innovative diagnostics on tissue biopsies
Tissue transcriptomics involves analyzing mRNA transcripts on biopsy tissue fragments using microarray technology, providing a quantitative and reproducible tool for graft biopsy analysis. The MMDX® molecular microscope, a microarray-based molecular diagnostic system, identified universal and specific mRNA changes associated with T-cell-mediated rejection (TCMR) and antibody-mediated rejection (ABMR), including interferon-γ (IFN-γ)-inducible genes. Different pathways and markers were defined for each rejection type. The Nanostring® B-HOT panel, another platform, categorized 770 genes relevant to rejection, tolerance, immune responses, and viral infections. The GoCAR study used the Nanostring technology to identify a gene set predicting progressive injury and fibrosis in kidney allografts, with superior predictive value compared to clinical and histology variables. These findings were validated in independent cohorts.
Non-invasive novel urinary biomarkers
Urine matrix is a promising substrate for developing biomarkers for organ rejection. Different methods have been used to study extracellular vesicles (EVs) in urine, which carry proteins, lipids, nucleic acids, and other bioactive molecules specific to the parent cell. Proteomic studies have identified urinary protein biomarkers associated with rejection. mRNA multigene signatures and miRNAs have also been studied as potential biomarkers. Urinary chemokines, such as CXCL10 and CXCL9, have shown promise in detecting rejection. Urinary metabolomics, which assesses kidney tissue metabolism, and urinary proteomics, which analyze a large number of proteins, have also been explored for rejection biomarkers. Combined “omics” approaches and artificial intelligence algorithms are being used to improve diagnostic accuracy. However, standardization and technological improvements are needed for widespread use of these biomarkers.
Non-invasive blood biomarkers
Several blood biomarkers have shown potential for clinical use in transplant rejection monitoring. Donor-derived cell-free DNA (cfDNA) has emerged as a promising biomarker, but technical challenges and defining a threshold for its quantification remain. Peripheral blood gene expression profiling has identified gene signatures that can predict rejection episodes, response to therapy, and graft loss. However, further validation and regulatory approval are necessary before widespread adoption. Blood proteomics, which aims to identify informative proteins associated with rejection, has encountered methodological limitations and requires extensive validation. Extracellular vesicles (EVs) derived from plasma have been explored as potential biomarkers, but their characterization and the prevalence of lymphoid-derived EVs present challenges that need to be addressed. Markers of immune status, such as virus-specific T cells (Tvis) and torque teno virus (TTV) load, offer insights into immunosuppression levels. Assessing Tvis against specific viruses allows personalized adjustment of immunosuppressive therapy, reducing overimmunosuppression and infection events. TTV load can serve as a simpler biomarker for immune status, aiding in optimizing drug dosage. Ongoing clinical trials are evaluating these approaches to further validate their utility.
Conclusions
Allorecognition is a complex phenomenon that cannot be thoroughly captured by the traditional biomarkers in use, which measure organ function, but generally fail to predict rejection before it becomes clinically evident. Recent experimental approaches have highlighted novel possibilities that will allow us to monitor graft health, modulate levels of immunosuppression, and ultimately to eliminate or reduce the need for protocol biopsies. Even if these approaches have been successful in several clinical trials, they still need to reach wide clinical application. This is particularly true in the pediatric setting, where the small patient numbers often preclude systematic testing of novel assays to diagnose rejection. Large and validated studies, addressing also the pediatric population, are therefore needed to take advantage of these highly versatile tools non-invasively and longitudinally over the long run.
References:
1. Sellares J, de Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, Hidalgo LG, Famulski K, Matas A, Halloran PF (2012) Understanding the causes of kidney transplant failure: the dominant role of antibody-mediated rejection and nonadherence. Am J Transplant 12:388–399.
2. Gordillo R, Munshi R, Monroe EJ, Shivaram GM, Smith JM (2019) Benefits and risks of protocol biopsies in pediatric renal transplantation. Pediatr Nephrol 34:593–598.
3. Barton KT, Halani K, Galbiati S, Dandamudi R, Hmiel SP, Dharnidharka VR, NAPRTCS investigators (2021) Late first acute rejection in pediatric kidney transplantation: a North American Pediatric Renal Trials and collaborative studies special study. Pediatr Transplant 25:e13953.
4. Kanzelmeyer NK, Lerch C, Ahlenstiel-Grunow T, Brasen JH, Haffner D, Pape L (2020) The role of protocol biopsies after pediatric kidney transplantation. Medicine (Baltimore) 99:e20522.
5. Moudgil A, Martz K, Stablein DM, Puliyanda DP (2010) Variables affecting estimated glomerular filtration rate after renal transplantation in children: a NAPRTCS data analysis. Pediatr Transplant 14:288–294.
6. Naesens M, Lerut E, Emonds MP, Herelixka A, Evenepoel P, Claes K, Bammens B, Sprangers B, Meijers B, Jochmans I, Monbaliu D, Pirenne J, Kuypers DR (2016) Proteinuria as a noninvasive marker for renal allograft histology and failure: an observational cohort study. J Am Soc Nephrol 27:281–292.
7. Kanzelmeyer NK, Ahlenstiel T, Drube J, Froede K, Kreuzer M, Broecker V, Ehrich JH, Melk A, Pape L (2010) Protocol biopsy-driven interventions after pediatric renal transplantation. Pediatr Transplant 14:1012–1018.


